In 2010, I wrote a series of blog posts on the health properties of potatoes (1, 2, 3). The evidence showed that potatoes are non-toxic, filling per calorie, remarkably nutritious, and can be eaten as almost the sole source of nutrition for extended periods of time (though I'm not recommending this). Traditional South American cultures such as the Quechua and Aymara have eaten potatoes as the major source of calories for generations without any apparent ill effects (3). This is particularly interesting since potatoes are one of the highest glycemic and most insulin-stimulating foods known.
Read more »
Wednesday, December 19, 2012
Friday, December 14, 2012
Thursday, December 13, 2012
Is it Time to Re-write the Textbooks on Insulin and Obesity? Part II
A new paper published on December 6th in the journal Science once again tackles the question of whether elevated insulin drives the development of obesity (1). Mice were generated that lack Jun kinases 1 and 2 specifically in immune cells, impairing their ability to produce inflammation while having very few off-target effects. These mice do not become insulin resistant when placed on a fattening diet, and their insulin levels do not increase one iota. Are they protected from obesity? People who read the last post should know the answer already.
Read more »
Read more »
Monday, December 10, 2012
Does tallness cause heart disease? No, but sex does
Popular beliefs about medical issues are sometimes motivated by a statistical phenomenon known as “spurious relationship”, among other names. Two variables X and Y are influenced by a third variable C, which leads to X and Y being correlated and thus the impression that X and Y are causally associated.
Take a look at the table below, which I blogged about in a previous post (). This table shows that there is a strong unadjusted correlation between height and arterial stiffness, a marker of heart disease. The likelihood that the correlation is due to chance is lower than one tenth of a percentage point (P<.001).
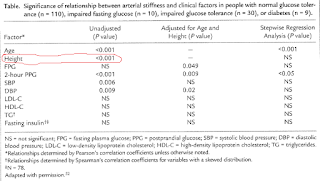
Interestingly, the authors of the study even use height as a control variable to narrow down the “true” causes of arterial stiffness (column with adjusted results), assuming that height did indeed influence arterial stiffness and what they found to be a key predictor of arterial stiffness, 2-hour postprandial glucose.
But there is no convincing evidence that height causes heart disease, with exception of pathological extremes – e.g., acromegaly. Extremes tend to influence statistical results somewhat, leading to conflicting conclusions that end up being disseminated by the popular media (). This is one of the sources of popular beliefs about medical issues.
Another, more important, source are real confounders. And this takes us back to the issue of height being associated with heart disease. In fact, height will typically be significantly associated with heart disease in almost any study that includes men and women and does not control for biological sex.
One of the reasons is that women overall tend to have a significantly lower incident of heart disease than men. The other is that height is significantly lower among women than men, on average, even though there are several women who are taller than the average man.
The table above was from a study including both sexes. Therefore, the strong association between height and arterial stiffness is a “reflection” of the strong association between being male and increased arterial stiffness. If one were to add a variable coded as 0 for male and 1 for female, and use it in a multivariate analysis of predictor of arterial stiffness, together with height, the effect of height would probably “disappear”.
Biological sex is the control variable, the “confounder”, that the authors should have used to narrow down the “true” causes of arterial stiffness (second column in the table). In the absence of biological sex, controlling for height accomplished something similar, but in a “wobbly” way, leaving many readers scratching their heads in confusion.
Take a look at the table below, which I blogged about in a previous post (). This table shows that there is a strong unadjusted correlation between height and arterial stiffness, a marker of heart disease. The likelihood that the correlation is due to chance is lower than one tenth of a percentage point (P<.001).

Interestingly, the authors of the study even use height as a control variable to narrow down the “true” causes of arterial stiffness (column with adjusted results), assuming that height did indeed influence arterial stiffness and what they found to be a key predictor of arterial stiffness, 2-hour postprandial glucose.
But there is no convincing evidence that height causes heart disease, with exception of pathological extremes – e.g., acromegaly. Extremes tend to influence statistical results somewhat, leading to conflicting conclusions that end up being disseminated by the popular media (). This is one of the sources of popular beliefs about medical issues.
Another, more important, source are real confounders. And this takes us back to the issue of height being associated with heart disease. In fact, height will typically be significantly associated with heart disease in almost any study that includes men and women and does not control for biological sex.
One of the reasons is that women overall tend to have a significantly lower incident of heart disease than men. The other is that height is significantly lower among women than men, on average, even though there are several women who are taller than the average man.
The table above was from a study including both sexes. Therefore, the strong association between height and arterial stiffness is a “reflection” of the strong association between being male and increased arterial stiffness. If one were to add a variable coded as 0 for male and 1 for female, and use it in a multivariate analysis of predictor of arterial stiffness, together with height, the effect of height would probably “disappear”.
Biological sex is the control variable, the “confounder”, that the authors should have used to narrow down the “true” causes of arterial stiffness (second column in the table). In the absence of biological sex, controlling for height accomplished something similar, but in a “wobbly” way, leaving many readers scratching their heads in confusion.
Friday, December 7, 2012

Thursday, December 6, 2012
Is it Time to Re-write the Textbooks on Insulin and Obesity?
A recent study in Cell Metabolism by Dr. Arya Mehran and colleagues found a result that, according to a press release, "could overturn widely accepted notions about healthy eating habits" (1), and has set the Internet abuzz.
In this study, researchers generated mice that lack one copy of the pancreatic insulin gene, and compared them to mice carrying both copies (2). Then, they exposed both groups to a fattening diet, and found that mice lacking one copy of the insulin gene secreted less insulin than the comparison group (i.e., they did not develop the same degree of hyperinsulinemia). These mice were also completely resistant to fat gain, while the comparison group became obese. The authors came to some rather large conclusions based on these results, suggesting that the "accepted model" that hyperinsulinemia is the result of obesity is "incompatible with our results that put the insulin hypersecretion genetically upstream of obesity". Ergo, diet causes hyperinsulinemia, which causes fat gain. It's a familiar argument to those who frequent Internet diet-health circles, except in this case the hyperinsulinemia is caused by a high-fat diet.
The problem is that the "accepted model" they want to replace overnight didn't come out of thin air-- it emerged from a large body of research, which was almost completely ignored by the authors. When carefully considered, this evidence suggests an alternative explanation for the results of Dr. Mehran and colleagues.
Read more »
In this study, researchers generated mice that lack one copy of the pancreatic insulin gene, and compared them to mice carrying both copies (2). Then, they exposed both groups to a fattening diet, and found that mice lacking one copy of the insulin gene secreted less insulin than the comparison group (i.e., they did not develop the same degree of hyperinsulinemia). These mice were also completely resistant to fat gain, while the comparison group became obese. The authors came to some rather large conclusions based on these results, suggesting that the "accepted model" that hyperinsulinemia is the result of obesity is "incompatible with our results that put the insulin hypersecretion genetically upstream of obesity". Ergo, diet causes hyperinsulinemia, which causes fat gain. It's a familiar argument to those who frequent Internet diet-health circles, except in this case the hyperinsulinemia is caused by a high-fat diet.
The problem is that the "accepted model" they want to replace overnight didn't come out of thin air-- it emerged from a large body of research, which was almost completely ignored by the authors. When carefully considered, this evidence suggests an alternative explanation for the results of Dr. Mehran and colleagues.
Read more »
Friday, November 30, 2012

Friday, November 23, 2012
Food Reward Friday
This week's winner: poutine!

While not as appetizing looking as the Monster Thickburger, poutine is probably more popular. For those who aren't familiar, poutine is a large plate of French fries, topped with gravy and cheese curds. It originated in Quebec, but has become popular throughout Canada and in the Northern US.
Read more »

While not as appetizing looking as the Monster Thickburger, poutine is probably more popular. For those who aren't familiar, poutine is a large plate of French fries, topped with gravy and cheese curds. It originated in Quebec, but has become popular throughout Canada and in the Northern US.
Read more »
Friday, November 16, 2012
Monday, November 12, 2012
The bipolar disorder pendulum: Depression as a compensatory adaptation
As far as explaining natural phenomena, Darwin was one of the best theoretical researchers of all time. Yet, there were a few phenomena that puzzled him for many years. One was the evolution of survival-impairing traits such as the peacock’s train, the large and brightly colored tail appendage observed in males.
Tha male peacock’s train is detrimental to the animal’s survival, and yet it is clearly an evolved trait ().
This type of trait is known as a “costly” trait – a trait that enhances biological fitness (or reproductive success, not to be confused with “gym fitness”), and yet is detrimental to the survival of the individuals who possess it (). Many costly traits have evolved in animals because of sexual selection. That is, they have evolved because they are sexy.
Costly traits seem like a contradiction in terms, but the mechanisms by which they can evolve become clear when evolution is modeled mathematically (, ). There is evidence that mental disorders may have evolved as costs of attractive mental traits (); one in particular, bipolar disorder (a.k.a. manic-depression), fits this hypothesis quite well.
Ironically, a key contributor to the mathematics used to understand costly traits, George R. Price (), might have suffered from severe bipolar disorder. Most of Price’s work in evolutionary biology was done in the 1970s; toward the end of his life, which was untimely ended by Price himself. For many years he was known mostly by evolutionary biologists, but this has changed recently with the publication of Oren Harman’s superb biographical book titled “The Price of Altruism: George Price and the Search for the Origins of Kindness” ().
Bipolar disorder is a condition characterized by disruptive mood swings. These swings are between manic and depressed states, and are analogous to the movement of a pendulum in that they alternate, seemingly gravitating around the "normal" state. See the figurative pendulum representation below, adapted from a drawing on Thinkquest.org.

Bipolar disorder is generally associated with creative intelligence, which is a very attractive trait (). Moreover, the manic state of the disorder is associated with hypersexuality and exaggerated generosity (). So one can clearly see how having bipolar disorder may lead to greater reproductive success, even as it creates long-term survival problems.
On one hand, a person may become very energetic and creative while in the manic state. This could be one of the reasons why many who suffer from bipolar disorder have fairly successful careers in fields that require creative intelligence (), which are many and not restricted to fields related to the fine and performing arts. Creative intelligence is highly valued in most knowledge-intensive professions ().
On the other hand, sustained acute mania or depression are frequently associated with serious health problems (). This is why the clinical treatment of bipolar disorder often starts with an attempt to keep the pendulum from moving too far in one direction or another. This may require medication, such as clinical doses of the elemental salt lithium, prior to cognitive behavioral therapy. The focus of cognitive behavioral therapy is on changing the way one sees and thinks about the world, particularly one’s “social world”.
Prolonged acute mania, usually accompanied by severely impaired sleep, may lead to psychosis. This, psychosis, is an extreme state characterized by hallucinations and/or delusions, leading to hospitalization in most cases. It has been theorized that depression is an involuntary compensatory adaptation () aimed at moving the pendulum in the other direction, out of the manic state, before more damage ensues ().
Elaborate approaches have been devised to treat and manage bipolar disorder treatment that involve the identification of mania and depression “prodromes” (), which are signs that a full-blown manic or depressive episode is about to start. Once prodromes are identified, cognitive behavioral therapy techniques are employed to prevent the pendulum from moving further in one direction or the other. The main goal of these techniques is to change one’s way of thinking about various issues (e.g., fears, pessimism). These techniques take years of practice to be used effectively.
Identification of prodromes and subsequent use of cognitive behavioral therapy seems to be particularly effective when dutifully applied with respect to manic episodes (). The reason for this may be related to one interesting fact related to bipolar disorder: manic episodes are not normally dreaded as much as depression episodes.
In fact, many sufferers avoid taking medication because they do not want to give up the creative and energetic bursts that come with manic episodes, even though they absolutely do not want the pendulum to go in the other direction. The problem is that, if depression is indeed a compensatory adaptation to mania, it seems reasonable to assume that extreme manic episodes are likely to be followed by extreme episodes of depression. Perhaps the key to avoid prolonged acute depression is to avoid prolonged acute mania.
As someone with bipolar disorder becomes more and more excited with novel and racing thoughts (a prodrome of mania), it would probably make sense to identify and carry out calming activities – to avoid a fall into despairing depression afterwards.
Tha male peacock’s train is detrimental to the animal’s survival, and yet it is clearly an evolved trait ().
This type of trait is known as a “costly” trait – a trait that enhances biological fitness (or reproductive success, not to be confused with “gym fitness”), and yet is detrimental to the survival of the individuals who possess it (). Many costly traits have evolved in animals because of sexual selection. That is, they have evolved because they are sexy.
Costly traits seem like a contradiction in terms, but the mechanisms by which they can evolve become clear when evolution is modeled mathematically (, ). There is evidence that mental disorders may have evolved as costs of attractive mental traits (); one in particular, bipolar disorder (a.k.a. manic-depression), fits this hypothesis quite well.
Ironically, a key contributor to the mathematics used to understand costly traits, George R. Price (), might have suffered from severe bipolar disorder. Most of Price’s work in evolutionary biology was done in the 1970s; toward the end of his life, which was untimely ended by Price himself. For many years he was known mostly by evolutionary biologists, but this has changed recently with the publication of Oren Harman’s superb biographical book titled “The Price of Altruism: George Price and the Search for the Origins of Kindness” ().
Bipolar disorder is a condition characterized by disruptive mood swings. These swings are between manic and depressed states, and are analogous to the movement of a pendulum in that they alternate, seemingly gravitating around the "normal" state. See the figurative pendulum representation below, adapted from a drawing on Thinkquest.org.

Bipolar disorder is generally associated with creative intelligence, which is a very attractive trait (). Moreover, the manic state of the disorder is associated with hypersexuality and exaggerated generosity (). So one can clearly see how having bipolar disorder may lead to greater reproductive success, even as it creates long-term survival problems.
On one hand, a person may become very energetic and creative while in the manic state. This could be one of the reasons why many who suffer from bipolar disorder have fairly successful careers in fields that require creative intelligence (), which are many and not restricted to fields related to the fine and performing arts. Creative intelligence is highly valued in most knowledge-intensive professions ().
On the other hand, sustained acute mania or depression are frequently associated with serious health problems (). This is why the clinical treatment of bipolar disorder often starts with an attempt to keep the pendulum from moving too far in one direction or another. This may require medication, such as clinical doses of the elemental salt lithium, prior to cognitive behavioral therapy. The focus of cognitive behavioral therapy is on changing the way one sees and thinks about the world, particularly one’s “social world”.
Prolonged acute mania, usually accompanied by severely impaired sleep, may lead to psychosis. This, psychosis, is an extreme state characterized by hallucinations and/or delusions, leading to hospitalization in most cases. It has been theorized that depression is an involuntary compensatory adaptation () aimed at moving the pendulum in the other direction, out of the manic state, before more damage ensues ().
Elaborate approaches have been devised to treat and manage bipolar disorder treatment that involve the identification of mania and depression “prodromes” (), which are signs that a full-blown manic or depressive episode is about to start. Once prodromes are identified, cognitive behavioral therapy techniques are employed to prevent the pendulum from moving further in one direction or the other. The main goal of these techniques is to change one’s way of thinking about various issues (e.g., fears, pessimism). These techniques take years of practice to be used effectively.
Identification of prodromes and subsequent use of cognitive behavioral therapy seems to be particularly effective when dutifully applied with respect to manic episodes (). The reason for this may be related to one interesting fact related to bipolar disorder: manic episodes are not normally dreaded as much as depression episodes.
In fact, many sufferers avoid taking medication because they do not want to give up the creative and energetic bursts that come with manic episodes, even though they absolutely do not want the pendulum to go in the other direction. The problem is that, if depression is indeed a compensatory adaptation to mania, it seems reasonable to assume that extreme manic episodes are likely to be followed by extreme episodes of depression. Perhaps the key to avoid prolonged acute depression is to avoid prolonged acute mania.
As someone with bipolar disorder becomes more and more excited with novel and racing thoughts (a prodrome of mania), it would probably make sense to identify and carry out calming activities – to avoid a fall into despairing depression afterwards.
Sunday, November 4, 2012
An Encouraging Trend
I was in the Seattle/Tacoma airport today, and I noticed quite a few people taking the stairs even though they're flanked by escalators. It's been my impression lately that more people are using stairs than even five years ago. I used to be the only weirdo on the stairs, but today I shared them with about ten other people. I know Seattle isn't necessarily representative of the nation as a whole, but I (optimistically) think of it as the vanguard in this respect.
One of the healthiest things a person can do is build exercise into daily life. You don't have to be Usain Bolt or Lance Armstrong to reap the benefits of exercise. In fact, evidence is accumulating that moderate exercise is healthier than extreme exercise. Taking the stairs instead of the elevator/escalator, walking or jogging even a modest amount, or standing for part of the day, can have an immediate, measurable impact on metabolic health (1).
Maybe it's macho, but I'll feel defeated the day I need a giant energy-guzzling machine to take me up a 15 foot incline. I have legs, and I intend to use them. Escalators are good for people who are disabled or have very heavy bags, but the rest of us have an opportunity to use our bodies in a natural and healthy way. Part of the problem is how buildings are designed. Humans tend to take the path of least resistance, and if the first thing we come across is an elevator, and the stairs are grimy and tucked away down some side hallway, we'll tend to take the elevator. Architects in some places are building in more prominent stairways to encourage gentle exercise throughout the day.
One of the healthiest things a person can do is build exercise into daily life. You don't have to be Usain Bolt or Lance Armstrong to reap the benefits of exercise. In fact, evidence is accumulating that moderate exercise is healthier than extreme exercise. Taking the stairs instead of the elevator/escalator, walking or jogging even a modest amount, or standing for part of the day, can have an immediate, measurable impact on metabolic health (1).
Maybe it's macho, but I'll feel defeated the day I need a giant energy-guzzling machine to take me up a 15 foot incline. I have legs, and I intend to use them. Escalators are good for people who are disabled or have very heavy bags, but the rest of us have an opportunity to use our bodies in a natural and healthy way. Part of the problem is how buildings are designed. Humans tend to take the path of least resistance, and if the first thing we come across is an elevator, and the stairs are grimy and tucked away down some side hallway, we'll tend to take the elevator. Architects in some places are building in more prominent stairways to encourage gentle exercise throughout the day.
Friday, November 2, 2012
Food Reward Friday
This week's lucky winner... the Hardee's MONSTER THICKBURGER!

Two 1/3 lb beef patties, four strips of bacon, three slices of American "cheese", mayo and bun. This bad boy boasts 1,300 calories, 830 from fat, 188 from carbohydrate and 228 from protein. Charred and fried processed meat, fake cheese, refined soybean oil mayo, and a white flour bun. You might as well just inject it directly into your carotid artery. Add a large fries and a medium coke, and you're at 2,110 calories. Who's hungry? Actually I am.
Read more »

Two 1/3 lb beef patties, four strips of bacon, three slices of American "cheese", mayo and bun. This bad boy boasts 1,300 calories, 830 from fat, 188 from carbohydrate and 228 from protein. Charred and fried processed meat, fake cheese, refined soybean oil mayo, and a white flour bun. You might as well just inject it directly into your carotid artery. Add a large fries and a medium coke, and you're at 2,110 calories. Who's hungry? Actually I am.
Read more »
Monday, October 29, 2012
The man who ate 25 eggs per day: What does this case really tell us?
Many readers of this blog have probably heard about the case of the man who ate approximately 25 eggs (20 to 30) per day for over 15 years (probably well over), was almost 90 years old (88) when the case was published in the prestigious The New England Journal of Medicine, and was in surprisingly good health ().
The case was authored by the late Dr. Fred Kern, Jr., a widely published lipid researcher after whom the Kern Lipid Conference is named (). One of Kern’s research interests was bile, a bitter-tasting fluid produced by the liver (and stored in the gallbladder) that helps with the digestion of lipids in the small intestine. He frames the man’s case in terms of a compensatory adaptation tied to bile secretion, arguing that this man was rather unique in his ability to deal with a lethal daily dose of dietary cholesterol.
Kern seemed to believe that dietary cholesterol was harmful, but that this man was somehow “immune” to it. This is ironic, because often this case is presented as evidence against the hypothesis that dietary cholesterol can be harmful. The table below shows the general nutrient content of the man’s daily diet of eggs. The numbers in this and other tables are based on data from Nutritiondata.com (), in some cases triangulated with other data. The 5.3 g of cholesterol in the table (i.e., 5,300 mg) is 1,775 percent the daily value recommended by the Institute of Medicine of the U.S. National Academy of Sciences ().

As you can see, the man was on a very low carbohydrate diet with a high daily intake of fat and protein. The man is described as an: “… 88-year-old man who lived in a retirement community [and] complained only of loneliness since his wife's death. He was an articulate, well-educated elderly man, healthy except for an extremely poor memory without other specific neurologic deficits … His general health had been excellent, without notable symptoms. He had mild constipation.”
The description does not suggest inherited high longevity: “His weight had been constant at 82 to 86 kg (height, 1.87 m). He had no history (according to the patient and his personal physician of 15 years) of heart disease, stroke, or kidney disease … The patient had never smoked and never drank excessively. His father died of unknown causes at the age of 40, and his mother died at 76 … He kept a careful record, egg by egg, of the number ingested each day …”
The table below shows the fat content of the man’s daily diet of eggs. With over 14 g of omega-6 fat intake every day, this man was probably close to or in “industrial seed oils territory” (), as far as daily omega-6 fat intake is concerned. And the intake of omega-3 fats, at less than 1 g, was not nearly enough to balance it. However, here is a relevant fact – this man was not consuming any industrial seed oils. He liked his eggs soft-boiled, which is why the numbers in this post refer to boiled eggs.

This man weighed between 82 to 86 kg, which is about 180 to 190 lbs. His height was 1.87 m, or about 6 ft 1 in. Therefore his body mass index varied between approximately 23 and 25, which is in the normal range. In other words, this person was not even close to obese during the many years he consumed 25 eggs or so per day. In the comments section of a previous post, on the sharp increase in obesity since the 1980s (), several readers argued that the sharp increase in obesity was very likely caused by an increase in omega-6 fat consumption.
I am open to the idea that industrialized omega-6 fats played a role in the sharp increase in obesity observed since the 1980s. When it comes to omega-6 fat consumption in general, including that in “more natural” foods (e.g., poultry and eggs), I am more skeptical. Still, it is quite possible that a diet high in omega-6 fats in general is unhealthy primarily if it is devoid of other nutrients. This man’s overall diet might have been protective not because of what he was not eating, but because of what he was eating.
The current debates pitting one diet against another often revolve around the ability of one diet or another to eliminate or reduce the intake of a “bad thing” (e.g., cholesterol, saturated fat, carbohydrates). Perhaps the discussion should be more focused on, or at least not completely ignore, what one diet or another include as protective factors. This would help better explain “odd findings”, such as the lowest-mortality body mass index of 26 in urban populations (). It would also help better explain “surprising cases”; such as this 25-eggs-a-day man’s, vegetarian-vegan “ageless woman” Annette Larkins’s (), and the decidedly carnivore De Vany couple’s ().
The table below shows the vitamin content of the man’s daily diet of eggs. The vitamin K2 content provided by Nutritiondata.com was incorrect; I had to get what seems to be the right number by triangulating values taken from various publications. And here we see something interesting. This man was consuming approximately the equivalent in vitamin K2 that one would get by eating 4 ounces of foie gras () every day. Foie gras, the fatty liver of overfed geese, is the richest known animal source of vitamin K2. This man’s diet was also high in vitamin A, which is believed to act synergistically with vitamin K2 – see Chris Masterjohn’s article on Weston Price’s “activator X” ().

Kern argued that the very high intake of dietary cholesterol led to a sharp increase in bile secretion, as the body tried to “get rid” of cholesterol (which is used in the synthesis of bile). However, the increased bile secretion might have been also been due to the high fat content of this man’s diet, since one of the main functions of bile is digestion of fats. Whatever the case may be, increased bile secretion leads to increased absorption of fat-soluble vitamins, and vitamins K2 and A are fat-soluble vitamins that seem to be protective against cardiovascular disease, cancer and other degenerative diseases.
Finally, the table below shows the mineral content of the man’s daily diet of eggs. As you can see, this man consumed 550 percent the officially recommended daily intake of selenium. This intake was slightly lower than the 400 micrograms per day purported to cause selenosis in adults (). Similarly to vitamins K2 and A, selenium seems to be protective against cardiovascular disease, cancer and other degenerative diseases. This man’s diet was also rich in phosphorus, needed for healthy teeth and bones.

Not too many people live to be 88 years of age; many fewer reach that age in fairly good health. The country with the highest average life expectancy in the world at the time of this writing is Japan, with a life expectancy of about 82 years (79 for men, and 86 for women). Those who think that they need a high HDL cholesterol and a low LDL cholesterol to be in good health, and thus live long lives, may be surprised at this man’s lipid profile: “The patient's plasma lipid levels were normal: total cholesterol, 5.18 mmol per liter (200 mg per deciliter); LDL, 3.68 mmol per liter (142 mg per deciliter); and HDL, 1.17 mmol per liter (45 mg per deciliter). The ratio of LDL to HDL cholesterol was 3.15.”
If we assume that this man is at least somewhat representative of the human species, and not a major exception as Kern argued, this case tells us that a diet of 25 eggs per day followed by over 15 years may actually be healthy for humans. Such diet has the following features:
- It is very high in dietary cholesterol.
- It involves a high intake of omega-6 fats from animal sources, with none coming from industrial seed oils.
- It involves a high overall intake of fats, including saturated fats.
- It is fairly high in protein, all of which from animal sources.
- It is a very low carbohydrate diet, with no sugar in it.
- It is a nutritious diet, rich in vitamins K2 and A, as well as in selenium and phosphorus.
This man ate 25 eggs per day apparently due to an obsession tied to mental problems. Repeated attempts at changing his behavior were unsuccessful. He said: “Eating these eggs ruins my life, but I can't help it.”
The case was authored by the late Dr. Fred Kern, Jr., a widely published lipid researcher after whom the Kern Lipid Conference is named (). One of Kern’s research interests was bile, a bitter-tasting fluid produced by the liver (and stored in the gallbladder) that helps with the digestion of lipids in the small intestine. He frames the man’s case in terms of a compensatory adaptation tied to bile secretion, arguing that this man was rather unique in his ability to deal with a lethal daily dose of dietary cholesterol.
Kern seemed to believe that dietary cholesterol was harmful, but that this man was somehow “immune” to it. This is ironic, because often this case is presented as evidence against the hypothesis that dietary cholesterol can be harmful. The table below shows the general nutrient content of the man’s daily diet of eggs. The numbers in this and other tables are based on data from Nutritiondata.com (), in some cases triangulated with other data. The 5.3 g of cholesterol in the table (i.e., 5,300 mg) is 1,775 percent the daily value recommended by the Institute of Medicine of the U.S. National Academy of Sciences ().

As you can see, the man was on a very low carbohydrate diet with a high daily intake of fat and protein. The man is described as an: “… 88-year-old man who lived in a retirement community [and] complained only of loneliness since his wife's death. He was an articulate, well-educated elderly man, healthy except for an extremely poor memory without other specific neurologic deficits … His general health had been excellent, without notable symptoms. He had mild constipation.”
The description does not suggest inherited high longevity: “His weight had been constant at 82 to 86 kg (height, 1.87 m). He had no history (according to the patient and his personal physician of 15 years) of heart disease, stroke, or kidney disease … The patient had never smoked and never drank excessively. His father died of unknown causes at the age of 40, and his mother died at 76 … He kept a careful record, egg by egg, of the number ingested each day …”
The table below shows the fat content of the man’s daily diet of eggs. With over 14 g of omega-6 fat intake every day, this man was probably close to or in “industrial seed oils territory” (), as far as daily omega-6 fat intake is concerned. And the intake of omega-3 fats, at less than 1 g, was not nearly enough to balance it. However, here is a relevant fact – this man was not consuming any industrial seed oils. He liked his eggs soft-boiled, which is why the numbers in this post refer to boiled eggs.

This man weighed between 82 to 86 kg, which is about 180 to 190 lbs. His height was 1.87 m, or about 6 ft 1 in. Therefore his body mass index varied between approximately 23 and 25, which is in the normal range. In other words, this person was not even close to obese during the many years he consumed 25 eggs or so per day. In the comments section of a previous post, on the sharp increase in obesity since the 1980s (), several readers argued that the sharp increase in obesity was very likely caused by an increase in omega-6 fat consumption.
I am open to the idea that industrialized omega-6 fats played a role in the sharp increase in obesity observed since the 1980s. When it comes to omega-6 fat consumption in general, including that in “more natural” foods (e.g., poultry and eggs), I am more skeptical. Still, it is quite possible that a diet high in omega-6 fats in general is unhealthy primarily if it is devoid of other nutrients. This man’s overall diet might have been protective not because of what he was not eating, but because of what he was eating.
The current debates pitting one diet against another often revolve around the ability of one diet or another to eliminate or reduce the intake of a “bad thing” (e.g., cholesterol, saturated fat, carbohydrates). Perhaps the discussion should be more focused on, or at least not completely ignore, what one diet or another include as protective factors. This would help better explain “odd findings”, such as the lowest-mortality body mass index of 26 in urban populations (). It would also help better explain “surprising cases”; such as this 25-eggs-a-day man’s, vegetarian-vegan “ageless woman” Annette Larkins’s (), and the decidedly carnivore De Vany couple’s ().
The table below shows the vitamin content of the man’s daily diet of eggs. The vitamin K2 content provided by Nutritiondata.com was incorrect; I had to get what seems to be the right number by triangulating values taken from various publications. And here we see something interesting. This man was consuming approximately the equivalent in vitamin K2 that one would get by eating 4 ounces of foie gras () every day. Foie gras, the fatty liver of overfed geese, is the richest known animal source of vitamin K2. This man’s diet was also high in vitamin A, which is believed to act synergistically with vitamin K2 – see Chris Masterjohn’s article on Weston Price’s “activator X” ().

Kern argued that the very high intake of dietary cholesterol led to a sharp increase in bile secretion, as the body tried to “get rid” of cholesterol (which is used in the synthesis of bile). However, the increased bile secretion might have been also been due to the high fat content of this man’s diet, since one of the main functions of bile is digestion of fats. Whatever the case may be, increased bile secretion leads to increased absorption of fat-soluble vitamins, and vitamins K2 and A are fat-soluble vitamins that seem to be protective against cardiovascular disease, cancer and other degenerative diseases.
Finally, the table below shows the mineral content of the man’s daily diet of eggs. As you can see, this man consumed 550 percent the officially recommended daily intake of selenium. This intake was slightly lower than the 400 micrograms per day purported to cause selenosis in adults (). Similarly to vitamins K2 and A, selenium seems to be protective against cardiovascular disease, cancer and other degenerative diseases. This man’s diet was also rich in phosphorus, needed for healthy teeth and bones.

Not too many people live to be 88 years of age; many fewer reach that age in fairly good health. The country with the highest average life expectancy in the world at the time of this writing is Japan, with a life expectancy of about 82 years (79 for men, and 86 for women). Those who think that they need a high HDL cholesterol and a low LDL cholesterol to be in good health, and thus live long lives, may be surprised at this man’s lipid profile: “The patient's plasma lipid levels were normal: total cholesterol, 5.18 mmol per liter (200 mg per deciliter); LDL, 3.68 mmol per liter (142 mg per deciliter); and HDL, 1.17 mmol per liter (45 mg per deciliter). The ratio of LDL to HDL cholesterol was 3.15.”
If we assume that this man is at least somewhat representative of the human species, and not a major exception as Kern argued, this case tells us that a diet of 25 eggs per day followed by over 15 years may actually be healthy for humans. Such diet has the following features:
- It is very high in dietary cholesterol.
- It involves a high intake of omega-6 fats from animal sources, with none coming from industrial seed oils.
- It involves a high overall intake of fats, including saturated fats.
- It is fairly high in protein, all of which from animal sources.
- It is a very low carbohydrate diet, with no sugar in it.
- It is a nutritious diet, rich in vitamins K2 and A, as well as in selenium and phosphorus.
This man ate 25 eggs per day apparently due to an obsession tied to mental problems. Repeated attempts at changing his behavior were unsuccessful. He said: “Eating these eggs ruins my life, but I can't help it.”
Friday, October 26, 2012
Food Reward Fridays
Each Friday, I'm going to post a picture of a modern food so ridiculous it makes you want to laugh and cry at the same time. I'm doing this for two reasons:
Read more »
- To raise awareness about the unhealthy, fattening foods that are taking over global food culture. These are highly rewarding, highly palatable, energy-dense foods that drive people to eat in the absence of hunger, and continue eating beyond calorie needs. In many cases, the foods have been specifically designed to maximize "craveability" and palatability.
- Because it's funny.
Without further ado... the first lucky winner:
Saturday, October 20, 2012
Candy at the Cash Register
Last week, the New England Journal of Medicine published an interesting editorial titled "Candy at the Cash Register-- a Risk Factor for Obesity and Chronic Disease." This fits in well with our discussion of non-homeostatic eating, or eating in the absence of calorie need.
There are a few quotes in this article that I find really perceptive.
Read more »
There are a few quotes in this article that I find really perceptive.
Read more »
Monday, October 15, 2012
The steep obesity increase in the USA in the 1980s: In a sense, it reflects a major success story
Obesity rates have increased in the USA over the years, but the steep increase starting around the 1980s is unusual. Wang and Beydoun do a good job at discussing this puzzling phenomenon (), and a blog post by Discover Magazine provides a graph (see below) that clear illustrates it ().

What is the reason for this?
You may be tempted to point at increases in calorie intake and/or changes in macronutrient composition, but neither can explain this sharp increase in obesity in the 1980s. The differences in calorie intake and macronutrient composition are simply not large enough to fully account for such a steep increase. And the data is actually full of oddities.
For example, an article by Austin and colleagues (which ironically blames calorie consumption for the obesity epidemic) suggests that obese men in a NHANES (2005–2006) sample consumed only 2.2 percent more calories per day on average than normal weight men in a NHANES I (1971–1975) sample ().
So, what could be the main reason for the steep increase in obesity prevalence since the 1980s?
The first clue comes from an interesting observation. If you age-adjust obesity trends (by controlling for age), you end up with a much less steep increase. The steep increase in the graph above is based on raw, unadjusted numbers. There is a higher prevalence of obesity among older people (no surprise here). And older people are people that have survived longer than younger people. (Don’t be too quick to say “duh” just yet.)
This age-obesity connection also reflects an interesting difference between humans living “in the wild” and those who do not, which becomes more striking when we compare hunter-gatherers with modern urbanites. Adult hunter-gatherers, unlike modern urbanites, do not gain weight as they age; they actually lose weight (, ).
Modern urbanites gain a significant amount of weight, usually as body fat, particularly after age 40. The table below, from an article by Flegal and colleagues, illustrates this pattern quite clearly (). Obesity prevalence tends to be highest between ages 40-59 in men; and this has been happening since the 1960s, with the exception of the most recent period listed (1999-2000).

In the 1999-2000 period obesity prevalence in men peaked in the 60-74 age range. Why? With progress in medicine, it is likely that more obese people in that age range survived (however miserably) in the 1999-2000 period. Obesity prevalence overall tends to be highest between ages 40-74 in women, which is a wider range than in men. Keep in mind that women tend to also live longer than men.
Because age seems to be associated with obesity prevalence among urbanites, it would be reasonable to look for a factor that significantly increased survival rates as one of the main reasons for the steep increase in the prevalence of obesity in the USA in the 1980s. If significantly more people were surviving beyond age 40 in the 1980s and beyond, this would help explain the steep increase in obesity prevalence. People don’t die immediately after they become obese; obesity is a “disease” that first and foremost impairs quality of life for many years before it kills.
Now look at the graph below, from an article by Armstrong and colleagues (). It shows a significant decrease in mortality from infectious diseases in the USA since 1900, reaching a minimum point between 1950 and 1960 (possibly 1955), and remaining low afterwards. (The spike in 1918 is due to the influenza pandemic.) At the same time, mortality from non-infectious diseases remains relatively stable over the same period, leading to a similar decrease in overall mortality.

When proper treatment options are not available, infectious diseases kill disproportionately at ages 15 and under (). Someone who was 15 years old in the USA in 1955 would have been 40 years old in 1980, if he or she survived. Had this person been obese, this would have been just in time to contribute to the steep increase in obesity trends in the USA. This increase would be cumulative; if this person were to live to the age of 70, he or she would be contributing to the obesity statistics up to 2010.
Americans are clearly eating more, particularly highly palatable industrialized foods whose calorie-to-nutrient ratio is high. Americans are also less physically active. But one of the fundamental reasons for the sharp increase in obesity rates in the USA since the early 1980s is that Americans have been surviving beyond age 40 in significantly greater numbers.
This is due to the success of modern medicine and public health initiatives in dealing with infectious diseases.
PS: It is important to point out that this post is not about the increase in American obesity in general over the years, but rather about the sharp increase in obesity since the early 1980s. A few alternative hypotheses have been proposed in the comments section, of which one seems to have been favored by various readers: a significant increase in consumption of linoleic acid (not to be confused with linolenic acid) since the early 1980s.

What is the reason for this?
You may be tempted to point at increases in calorie intake and/or changes in macronutrient composition, but neither can explain this sharp increase in obesity in the 1980s. The differences in calorie intake and macronutrient composition are simply not large enough to fully account for such a steep increase. And the data is actually full of oddities.
For example, an article by Austin and colleagues (which ironically blames calorie consumption for the obesity epidemic) suggests that obese men in a NHANES (2005–2006) sample consumed only 2.2 percent more calories per day on average than normal weight men in a NHANES I (1971–1975) sample ().
So, what could be the main reason for the steep increase in obesity prevalence since the 1980s?
The first clue comes from an interesting observation. If you age-adjust obesity trends (by controlling for age), you end up with a much less steep increase. The steep increase in the graph above is based on raw, unadjusted numbers. There is a higher prevalence of obesity among older people (no surprise here). And older people are people that have survived longer than younger people. (Don’t be too quick to say “duh” just yet.)
This age-obesity connection also reflects an interesting difference between humans living “in the wild” and those who do not, which becomes more striking when we compare hunter-gatherers with modern urbanites. Adult hunter-gatherers, unlike modern urbanites, do not gain weight as they age; they actually lose weight (, ).
Modern urbanites gain a significant amount of weight, usually as body fat, particularly after age 40. The table below, from an article by Flegal and colleagues, illustrates this pattern quite clearly (). Obesity prevalence tends to be highest between ages 40-59 in men; and this has been happening since the 1960s, with the exception of the most recent period listed (1999-2000).

In the 1999-2000 period obesity prevalence in men peaked in the 60-74 age range. Why? With progress in medicine, it is likely that more obese people in that age range survived (however miserably) in the 1999-2000 period. Obesity prevalence overall tends to be highest between ages 40-74 in women, which is a wider range than in men. Keep in mind that women tend to also live longer than men.
Because age seems to be associated with obesity prevalence among urbanites, it would be reasonable to look for a factor that significantly increased survival rates as one of the main reasons for the steep increase in the prevalence of obesity in the USA in the 1980s. If significantly more people were surviving beyond age 40 in the 1980s and beyond, this would help explain the steep increase in obesity prevalence. People don’t die immediately after they become obese; obesity is a “disease” that first and foremost impairs quality of life for many years before it kills.
Now look at the graph below, from an article by Armstrong and colleagues (). It shows a significant decrease in mortality from infectious diseases in the USA since 1900, reaching a minimum point between 1950 and 1960 (possibly 1955), and remaining low afterwards. (The spike in 1918 is due to the influenza pandemic.) At the same time, mortality from non-infectious diseases remains relatively stable over the same period, leading to a similar decrease in overall mortality.

When proper treatment options are not available, infectious diseases kill disproportionately at ages 15 and under (). Someone who was 15 years old in the USA in 1955 would have been 40 years old in 1980, if he or she survived. Had this person been obese, this would have been just in time to contribute to the steep increase in obesity trends in the USA. This increase would be cumulative; if this person were to live to the age of 70, he or she would be contributing to the obesity statistics up to 2010.
Americans are clearly eating more, particularly highly palatable industrialized foods whose calorie-to-nutrient ratio is high. Americans are also less physically active. But one of the fundamental reasons for the sharp increase in obesity rates in the USA since the early 1980s is that Americans have been surviving beyond age 40 in significantly greater numbers.
This is due to the success of modern medicine and public health initiatives in dealing with infectious diseases.
PS: It is important to point out that this post is not about the increase in American obesity in general over the years, but rather about the sharp increase in obesity since the early 1980s. A few alternative hypotheses have been proposed in the comments section, of which one seems to have been favored by various readers: a significant increase in consumption of linoleic acid (not to be confused with linolenic acid) since the early 1980s.
Thursday, October 4, 2012
Photos and More Gardening
I've needed new professional and blog photos for a long time. My friend Adam Roe was in town recently, and he happens to be professional photographer, so he graciously offered to snap a few shots. Despite less than ideal conditions, he did an outstanding job. Here's a larger version of the photo on my profile (which Blogger shrinks down to a tiny thumbnail):

To see more of Adam's work, head over to his Facebook page, and don't forget to 'like' and share it if you enjoy it. Adam is currently based in Berlin.
Gardening Update
Here's a photo of today's harvest (taken by me, not Adam; you can tell by the poor focus and primitive lighting):
Read more »

To see more of Adam's work, head over to his Facebook page, and don't forget to 'like' and share it if you enjoy it. Adam is currently based in Berlin.
Gardening Update
Here's a photo of today's harvest (taken by me, not Adam; you can tell by the poor focus and primitive lighting):
Read more »
Monday, October 1, 2012
The anatomy of a VAP test report
The vertical auto profile (VAP) test is an enhanced lipid profile test. It has been proposed, chiefly by the company Atherotech (), as a more complete test that relies on direct measurement of previously calculated lipid measures. The VAP test is particularly known for providing direct measurements of LDL cholesterol, instead of calculating them through equations ().
At the time of this writing, a typical VAP test report would provide direct measures of the cholesterol content of LDL, Lp(a), IDL, HDL, and VLDL particles. It would also provide additional measures referred to as secondary risk factors, notably particle density patterns and apolipoprotein concentrations. Finally, it would provide a customized risk summary and some basic recommendations for treatment. Below is the top part of a typical VAP test report (from Atherotech), showing measures of the cholesterol content of various particles. LDL cholesterol is combined for four particle subtypes, the small-dense subtypes 4 and 3, and the large-buoyant subtypes 2 and 1. A breakdown by LDL particle subtype is provided later in the VAP report.

In the table above, HDL cholesterol is categorized in two subtypes, the small-dense subtype 2, and the large-buoyant subtype 3. Interestingly, most of the HDL cholesterol in the table is supposedly of the least protective subtype, which seems to be a common finding in the general population. VLDL cholesterol is categorized in a similar way. IDL stands for intermediate-density lipoprotein; this is essentially a VLDL particle that has given off some of its content, particularly its triglyceride (or fat) cargo, but still remains in circulation.
Lp(a) is a special subtype of the LDL particle that is purported to be associated with markedly atherogenic factors. Mainstream medicine generally considers Lp(a) particles themselves to be atherogenic, which is highly debatable. Among other things, cardiovascular disease (CVD) risk and Lp(a) concentration follow a J-curve pattern, and Lp(a)’s range of variation in humans is very large. A blog post by Peter (Hyperlipid) has a figure right at the top that illustrates the former J-curve assertion (). The latter fact, related to range of variation, generally leads to a rather wide normal distribution of Lp(a) concentrations in most populations; meaning that a large number of individuals tend to fall outside Lp(a)’s optimal range and still have a low risk of developing CVD.
Below is the middle part of a typical VAP report, showing secondary risk factors, such as particle density patterns and apolipoprotein concentrations. LDL particle pattern A is considered to be the most protective, supposedly because large-buoyant LDL particles are less likely to penetrate the endothelial gaps, which are about 25 nm in diameter. Apolipoproteins are proteins that bind to fats for their transport in lipoproteins, to be used by various tissues for energy; free fatty acids also need to bind to proteins, notably albumin, to be transported to tissues for use as energy. Redundant particles and processes are everywhere in the human body!

Below is the bottom part of a typical VAP report, providing a risk summary and some basic recommendations. One of the recommendations is “to lower” the LDL target from 130mg/dL to 100mg/dL due to the presence of the checked emerging risk factors on the right, under “Considerations”. What that usually means in practice is a recommendation to take drugs, especially statins, to reduce LDL cholesterol levels. A recent post here and the discussion under it suggest that this would be a highly questionable recommendation in the vast majority of cases ().

What do I think about VAP tests? I think that they are useful in that they provide a lot more information about one’s lipids than standard lipid profiles, and more information is better than less. On the other hand, I think that people should be very careful about what they do with that information. There are even more direct tests that I would recommend before a decision to take drugs is made (, ), if that decision is ever made at all.
At the time of this writing, a typical VAP test report would provide direct measures of the cholesterol content of LDL, Lp(a), IDL, HDL, and VLDL particles. It would also provide additional measures referred to as secondary risk factors, notably particle density patterns and apolipoprotein concentrations. Finally, it would provide a customized risk summary and some basic recommendations for treatment. Below is the top part of a typical VAP test report (from Atherotech), showing measures of the cholesterol content of various particles. LDL cholesterol is combined for four particle subtypes, the small-dense subtypes 4 and 3, and the large-buoyant subtypes 2 and 1. A breakdown by LDL particle subtype is provided later in the VAP report.

In the table above, HDL cholesterol is categorized in two subtypes, the small-dense subtype 2, and the large-buoyant subtype 3. Interestingly, most of the HDL cholesterol in the table is supposedly of the least protective subtype, which seems to be a common finding in the general population. VLDL cholesterol is categorized in a similar way. IDL stands for intermediate-density lipoprotein; this is essentially a VLDL particle that has given off some of its content, particularly its triglyceride (or fat) cargo, but still remains in circulation.
Lp(a) is a special subtype of the LDL particle that is purported to be associated with markedly atherogenic factors. Mainstream medicine generally considers Lp(a) particles themselves to be atherogenic, which is highly debatable. Among other things, cardiovascular disease (CVD) risk and Lp(a) concentration follow a J-curve pattern, and Lp(a)’s range of variation in humans is very large. A blog post by Peter (Hyperlipid) has a figure right at the top that illustrates the former J-curve assertion (). The latter fact, related to range of variation, generally leads to a rather wide normal distribution of Lp(a) concentrations in most populations; meaning that a large number of individuals tend to fall outside Lp(a)’s optimal range and still have a low risk of developing CVD.
Below is the middle part of a typical VAP report, showing secondary risk factors, such as particle density patterns and apolipoprotein concentrations. LDL particle pattern A is considered to be the most protective, supposedly because large-buoyant LDL particles are less likely to penetrate the endothelial gaps, which are about 25 nm in diameter. Apolipoproteins are proteins that bind to fats for their transport in lipoproteins, to be used by various tissues for energy; free fatty acids also need to bind to proteins, notably albumin, to be transported to tissues for use as energy. Redundant particles and processes are everywhere in the human body!

Below is the bottom part of a typical VAP report, providing a risk summary and some basic recommendations. One of the recommendations is “to lower” the LDL target from 130mg/dL to 100mg/dL due to the presence of the checked emerging risk factors on the right, under “Considerations”. What that usually means in practice is a recommendation to take drugs, especially statins, to reduce LDL cholesterol levels. A recent post here and the discussion under it suggest that this would be a highly questionable recommendation in the vast majority of cases ().

What do I think about VAP tests? I think that they are useful in that they provide a lot more information about one’s lipids than standard lipid profiles, and more information is better than less. On the other hand, I think that people should be very careful about what they do with that information. There are even more direct tests that I would recommend before a decision to take drugs is made (, ), if that decision is ever made at all.
Monday, September 17, 2012
Familial hypercholesteromia: Why rely on cholesterol levels when more direct measures are available?
There are two forms of familial hypercholesteromia (FH), namely heterozygous and homozygous FH. In heterozygous FH only one copy of the gene that causes it is present, inherited either from the father or the mother. In homozygous FH, which is the most lethal form, two copies of the gene are present. FH is associated with early-onset cardiovascular disease (CVD).
Homozygous FH may happen if both the father and mother have heterozygous or homozygous FH. If both the father and mother have heterozygous FH, the likelihood that at least one in four children will have homozygous FH will be high. If both parents have homozygous FH the likelihood that all children will have homozygous FH will be high.
In fact, in the latter case, homozygous FH in the children is almost certain. One case in which it won’t occur is if the combining FH gene from the father or mother mutates into a non-FH gene before it is used in the assembly of the genome of the child. A gene mutation in a specific locus, only for the father or mother, is an unlikely event, and would lead to heterozygous FH. Two gene mutations at once in the same locus, for the father and mother, is a very unlikely event.
By the way, despite what many are led to believe based on fictional characters in movies and series like the X-Men and Hulk, mutations in functional genes usually lead to harmful traits. In our evolutionary past, those traits would have been largely removed from the gene pool by selection, making them rare or nonexistent in modern humans. Today we have modern medicine; a double-edged sword.
Mutations leading to super-human traits are very, very unlikely. The myostatin gene, for example, suppresses muscle growth. And yet the mutations that lead to little or no secretion of the related myostatin protein are very uncommon. Obviously they have not been favored by selection, even though their holders are very muscular – e.g., Germany’s “Incredible Hulky” ().
Okay, back to FH. Xanthelasmas are relatively common among those who suffer from FH (see photo below, from Globalskinatlas.com). They are skin deposits of cholesterol, have a genetic basis, and are NOT always associated with FH. This is important – several people have xanthelasmas but not FH.

FH is a fairly rare disease, even in its heterozygous form, with an overall incidence of approximately 0.2 percent. That is, about 1 in 500 people in the general population will have it. Genetically related groups will see a much higher or lower rate of incidence, as the disease is strongly influenced by a genetic mutation. This genetic mutation is apparently in the LDL receptor gene, located on the short arm of chromosome 19.
The table below, from a study by Miltiadous and colleagues (), paints a broad picture of the differences one would typically see between heterozygous FH sufferers and non-FH controls.

The main difference is in total cholesterol and in the relatively large contribution of LDL to total cholesterol. A large difference is also seen in Apolipoprotein B (indicated as "Apo B"), which acts as a LDL transporter (not to be confused with a LDL receptor). The LDL cholesterol shown on the table is calculated through the Friedewald equation, which is notoriously imprecise at low triglyceride levels ().
Looking at the total cholesterol row on the table, and assuming that the numbers after the plus/minus signs are standard deviations, we can conclude that: (a) a little more than two-thirds of the heterozygous FH sufferers had total cholesterol levels falling in between 280 and 446; and (b) a little more than two-thirds of the non-FH controls had total cholesterol levels falling in between 135 and 225.
Keep in mind that about 13.5 percent {calculated as: (95-68)/2} of the non-FH controls had total cholesterol levels between 225 and 270. This is a nontrivial percentage; i.e., these may be a minority but are not rare individuals. Heterozygous FH sufferers are rare, at 0.2 percent of the general population. Moreover, about 2 percent of the non-FH controls had non-pathological total cholesterol levels between 270 and 315. That is not so rare either, amounting to an “incidence” 10 times higher than heterozygous FH.
What would happen if people with heterozygous FH were to replace refined carbohydrates and sugars with saturated fat and cholesterol in their diets? Very likely their already high total cholesterol would go up higher, in part because their HDL cholesterol would go up (). Still, how could they be sure that CVD progression would accelerate if they did that?
According to some studies, the higher HDL cholesterol would either be generally protective or associated with protective factors, even among those with FH (). One of those protective factors may be a more nutrient-dense diet, as many foods rich in cholesterol are very nutrient-dense – e.g., eggs, organ meats, and seafood.
This brings me to my main point in this post. It is mainstream practice to diagnose people with FH based on total and/or LDL cholesterol levels. But the main problem with FH is that it leads to early onset of CVD, which can be measured more directly through simple tests, such as intima-media thickness and related ultrasound plaque tests (). These are noninvasive tests, done in 5 minutes or so, and often covered by insurance.
Even if simple direct tests are not perfect, it seems utterly nonsensical to rely on cholesterol measures to diagnose and treat FH, given the possible overlap between pathological and non-pathological high total cholesterol levels.
Homozygous FH may happen if both the father and mother have heterozygous or homozygous FH. If both the father and mother have heterozygous FH, the likelihood that at least one in four children will have homozygous FH will be high. If both parents have homozygous FH the likelihood that all children will have homozygous FH will be high.
In fact, in the latter case, homozygous FH in the children is almost certain. One case in which it won’t occur is if the combining FH gene from the father or mother mutates into a non-FH gene before it is used in the assembly of the genome of the child. A gene mutation in a specific locus, only for the father or mother, is an unlikely event, and would lead to heterozygous FH. Two gene mutations at once in the same locus, for the father and mother, is a very unlikely event.
By the way, despite what many are led to believe based on fictional characters in movies and series like the X-Men and Hulk, mutations in functional genes usually lead to harmful traits. In our evolutionary past, those traits would have been largely removed from the gene pool by selection, making them rare or nonexistent in modern humans. Today we have modern medicine; a double-edged sword.
Mutations leading to super-human traits are very, very unlikely. The myostatin gene, for example, suppresses muscle growth. And yet the mutations that lead to little or no secretion of the related myostatin protein are very uncommon. Obviously they have not been favored by selection, even though their holders are very muscular – e.g., Germany’s “Incredible Hulky” ().
Okay, back to FH. Xanthelasmas are relatively common among those who suffer from FH (see photo below, from Globalskinatlas.com). They are skin deposits of cholesterol, have a genetic basis, and are NOT always associated with FH. This is important – several people have xanthelasmas but not FH.

FH is a fairly rare disease, even in its heterozygous form, with an overall incidence of approximately 0.2 percent. That is, about 1 in 500 people in the general population will have it. Genetically related groups will see a much higher or lower rate of incidence, as the disease is strongly influenced by a genetic mutation. This genetic mutation is apparently in the LDL receptor gene, located on the short arm of chromosome 19.
The table below, from a study by Miltiadous and colleagues (), paints a broad picture of the differences one would typically see between heterozygous FH sufferers and non-FH controls.

The main difference is in total cholesterol and in the relatively large contribution of LDL to total cholesterol. A large difference is also seen in Apolipoprotein B (indicated as "Apo B"), which acts as a LDL transporter (not to be confused with a LDL receptor). The LDL cholesterol shown on the table is calculated through the Friedewald equation, which is notoriously imprecise at low triglyceride levels ().
Looking at the total cholesterol row on the table, and assuming that the numbers after the plus/minus signs are standard deviations, we can conclude that: (a) a little more than two-thirds of the heterozygous FH sufferers had total cholesterol levels falling in between 280 and 446; and (b) a little more than two-thirds of the non-FH controls had total cholesterol levels falling in between 135 and 225.
Keep in mind that about 13.5 percent {calculated as: (95-68)/2} of the non-FH controls had total cholesterol levels between 225 and 270. This is a nontrivial percentage; i.e., these may be a minority but are not rare individuals. Heterozygous FH sufferers are rare, at 0.2 percent of the general population. Moreover, about 2 percent of the non-FH controls had non-pathological total cholesterol levels between 270 and 315. That is not so rare either, amounting to an “incidence” 10 times higher than heterozygous FH.
What would happen if people with heterozygous FH were to replace refined carbohydrates and sugars with saturated fat and cholesterol in their diets? Very likely their already high total cholesterol would go up higher, in part because their HDL cholesterol would go up (). Still, how could they be sure that CVD progression would accelerate if they did that?
According to some studies, the higher HDL cholesterol would either be generally protective or associated with protective factors, even among those with FH (). One of those protective factors may be a more nutrient-dense diet, as many foods rich in cholesterol are very nutrient-dense – e.g., eggs, organ meats, and seafood.
This brings me to my main point in this post. It is mainstream practice to diagnose people with FH based on total and/or LDL cholesterol levels. But the main problem with FH is that it leads to early onset of CVD, which can be measured more directly through simple tests, such as intima-media thickness and related ultrasound plaque tests (). These are noninvasive tests, done in 5 minutes or so, and often covered by insurance.
Even if simple direct tests are not perfect, it seems utterly nonsensical to rely on cholesterol measures to diagnose and treat FH, given the possible overlap between pathological and non-pathological high total cholesterol levels.
Friday, September 14, 2012
More Thoughts on Macronutrient Trends
I had a brief positive exchange with Gary Taubes about the NuSI post. He reminded me that there's an artifact (measurement error) in the USDA data on fat consumption in the year 2000 when they changed assessment methods. Here are the USDA data on macronutrient consumption since 1970, corrected for loss (28.8%) but not corrected for the artifact:
 Read more »
Read more »

Wednesday, September 12, 2012
Nutrition Science Initiative (NuSI)
Some of you may have heard of an ambitious new nutrition research foundation called the Nutrition Science Initiative (NuSI). In this post, I'll explain what it is, why it matters, and how I feel about it-- from the perspective of an obesity researcher.
Monday, September 10, 2012
Calories and Carbohydrate: a Natural Experiment
In the lab, we work hard to design experiments that help us understand the natural world. But sometimes, nature sets up experiments for us, and all we have to do is collect the data. These are called "natural experiments", and they have led to profound insights in every field of science. For example, Alzheimer's disease is usually not considered a genetic disorder. However, researchers have identified rare cases where AD is inherited in a simple genetic manner. By identifying the genes involved, and what they do, we were able to increase our understanding of the molecular mechanisms of the disease.
The natural experiment I'll be discussing today began in 1989 with the onset of a major economic crisis in Cuba. This coincided with the loss of the Soviet Union as a trading partner, resulting in a massive economic collapse over the next six years, which gradually recovered by 2000.
Read more »
The natural experiment I'll be discussing today began in 1989 with the onset of a major economic crisis in Cuba. This coincided with the loss of the Soviet Union as a trading partner, resulting in a massive economic collapse over the next six years, which gradually recovered by 2000.
Read more »
Wednesday, September 5, 2012
A Late Summer Harvest
It's been a good year for gardening in Seattle, at least in my garden. Thanks to great new tools* and Steve Solomon's recipe for homemade fertilizer, my house has been swimming in home-grown vegetables all summer. I'm fortunate that a friend lets me garden a 300 square foot plot behind her house. Here's a photo of part of today's harvest; various kale/collards, zucchini, tomatoes and the last of the pole beans:

Perfect for the Eocene diet.
Read more »

Perfect for the Eocene diet.
Read more »
Monday, September 3, 2012
Daniel Suelo, the man who quit money, seems remarkably healthy
Daniel James Shellabarger (better known as Daniel Suelo) is portrayed in the bestselling 2012 nonfiction book by Mark Sundeen titled “The Man Who Quit Money” ().
Apparently Suelo stopped using money in 2000, and lives in a cave near the city of Moab in Utah. His diet comprises primarily wild vegetables and fruits, insects, and road kill; as well as discarded or donated food he gets from others when he visits the city. The photo below is from a recent BBC documentary. An interesting 2006 YouTube clip on Suelo is titled “Moneyless in Moab” ().

Suelo is listed as having been born in 1961 (), and the photo above appears to have been taken in 2012. If these dates are correct, he is 51 in the photo above. I cannot help but think that he looks remarkably healthy. The 40-50 age period is one that often sets the stage for many diseases of civilization in urban societies.
Suelo’s decision seems like a radical one, at least to me. There are always complex motivations behind radical decisions. In the case of Suelo, some of these motivations are captured in the comment below, which is part of a review of the book “The Man Who Quit Money” posted on Amazon.com by a reader.
Many people have been inspired by Suelo’s story, to some extent because they see that adopting a radical form of “simple living” () may not only be possible but also liberating. Obviously Suelo’s lifestyle, as it is now, would not be possible without the help of others who adopt a more “traditional” lifestyle. Below is a critical review by a reader of the book, posted on Amazon.com, which harshly reflects this perspective.
Still, Suelo’s story is interesting, including from a human health perspective. An article on Details.com by Christopher Ketcham provides a glimpse at what a day in Suelo’s life looks like (). It seems that on most days he has one main meal per day.
It is hard to get a sense of the nutrient composition of his diet. It looks like his diet is limited in but not devoid of industrial foods, and one in which food consumption is sporadic, opportunistic, and driven primarily by hunger and availability – not by stress or set meal times, for example.
He probably walks a lot; his cave is one hour away from Moab by foot, and it looks like he goes to Moab often. Apparently he almost never gets sick.
Suelo also writes a blog (), which has many followers, and also maintains other websites, from the Public Library in Moab. His first blog post has over 1,000 comments under it ().
Apparently Suelo stopped using money in 2000, and lives in a cave near the city of Moab in Utah. His diet comprises primarily wild vegetables and fruits, insects, and road kill; as well as discarded or donated food he gets from others when he visits the city. The photo below is from a recent BBC documentary. An interesting 2006 YouTube clip on Suelo is titled “Moneyless in Moab” ().

Suelo is listed as having been born in 1961 (), and the photo above appears to have been taken in 2012. If these dates are correct, he is 51 in the photo above. I cannot help but think that he looks remarkably healthy. The 40-50 age period is one that often sets the stage for many diseases of civilization in urban societies.
Suelo’s decision seems like a radical one, at least to me. There are always complex motivations behind radical decisions. In the case of Suelo, some of these motivations are captured in the comment below, which is part of a review of the book “The Man Who Quit Money” posted on Amazon.com by a reader.
[…] a picture of Suelo not as an untarnished hero, but a man who has wrestled with heartbreak, depression, disillusionment with his family's faith, and his repugnance to working for the pure sake of making money and buying things. Whether or not you are inspired to follow Suelo's example, this book will make you think.
Many people have been inspired by Suelo’s story, to some extent because they see that adopting a radical form of “simple living” () may not only be possible but also liberating. Obviously Suelo’s lifestyle, as it is now, would not be possible without the help of others who adopt a more “traditional” lifestyle. Below is a critical review by a reader of the book, posted on Amazon.com, which harshly reflects this perspective.
Any infantile mentality charmed by this inane story should simply generalize the message - visualize a world in which all of us live like the parasitic protagonist. How fortunate for Suelo that there are still people who engage in productive work and indirectly and unknowingly keep the human sponge alive […] Suelo never quit money he simply quit contributing anything and continues to survive simply as a parasite.
Still, Suelo’s story is interesting, including from a human health perspective. An article on Details.com by Christopher Ketcham provides a glimpse at what a day in Suelo’s life looks like (). It seems that on most days he has one main meal per day.
It is hard to get a sense of the nutrient composition of his diet. It looks like his diet is limited in but not devoid of industrial foods, and one in which food consumption is sporadic, opportunistic, and driven primarily by hunger and availability – not by stress or set meal times, for example.
He probably walks a lot; his cave is one hour away from Moab by foot, and it looks like he goes to Moab often. Apparently he almost never gets sick.
Suelo also writes a blog (), which has many followers, and also maintains other websites, from the Public Library in Moab. His first blog post has over 1,000 comments under it ().
Wednesday, August 29, 2012
Does Calorie Restriction Extend Lifespan in Mammals?
Until about two years ago, the story went something like this: calorie restriction extends lifespan in yeast, worms, flies, and rodents. Lifespan extension by calorie restriction appears to be biologically universal, therefore it's probably only a matter of time until it's demonstrated in humans as well. More than 20 years ago, independent teams of researchers set out to demonstrate the phenomenon in macaque monkeys, a primate model closer to humans than any lifespan model previously tested.
Recent findings have caused me to seriously question this narrative. One of the first challenges was the finding that genetically wild mice (as opposed to inbred laboratory strains) do not live longer when their calorie intake is restricted, despite showing hormonal changes associated with longevity in other strains, although the restricted animals do develop less cancer (1). One of the biggest blows came in 2009, when researchers published the results of a study that analyzed the effect of calorie restriction on lifespan in 41 different strains of mice, both male and female (2). They found that calorie restriction extends lifespan in a subset of strains, but actually shortens lifespan in an even larger subset. Below is a graph of the effect of calorie restriction on lifespan in the 41 strains. Positive numbers indicate that calorie restriction extended life, while negative numbers indicate that it shortened life:
Read more »
Recent findings have caused me to seriously question this narrative. One of the first challenges was the finding that genetically wild mice (as opposed to inbred laboratory strains) do not live longer when their calorie intake is restricted, despite showing hormonal changes associated with longevity in other strains, although the restricted animals do develop less cancer (1). One of the biggest blows came in 2009, when researchers published the results of a study that analyzed the effect of calorie restriction on lifespan in 41 different strains of mice, both male and female (2). They found that calorie restriction extends lifespan in a subset of strains, but actually shortens lifespan in an even larger subset. Below is a graph of the effect of calorie restriction on lifespan in the 41 strains. Positive numbers indicate that calorie restriction extended life, while negative numbers indicate that it shortened life:
Read more »
Wednesday, August 22, 2012
AHS11 Talk Posted
After a one-year delay, my talk from the 2011 Ancestral Health Symposium is online with slides synched. The talk is titled "Obesity: Old Solutions for a New Problem", and it's an overview of some of the research linking food reward to food intake and body fatness. This is the talk that introduced a fundamentally new idea to the ancestral community: not only does the chemical composition of food matter, but also its sensory qualities-- in fact, the sensory qualities of food are among the primary determinants of food intake. I didn't come up with the idea of course, I simply translated the research for a more general audience and put my own evolutionary spin on it.
The talk would be a bit different if I were to give it today, as my understanding of the subject has expanded, and my speaking skills have improved. However, the central message remains as true today as it was a year ago. You can find the talk here.
The slide synching was done by an extremely generous man named Ben Fury. As you can see in the video, he did an excellent job. Without Ben, this video would have remained in internet limbo forever.
Below, I've published a message from Ben explaining the interesting work that he does. Please contact him if you think it's interesting.
A Message from Ben Fury
The talk would be a bit different if I were to give it today, as my understanding of the subject has expanded, and my speaking skills have improved. However, the central message remains as true today as it was a year ago. You can find the talk here.
The slide synching was done by an extremely generous man named Ben Fury. As you can see in the video, he did an excellent job. Without Ben, this video would have remained in internet limbo forever.
Below, I've published a message from Ben explaining the interesting work that he does. Please contact him if you think it's interesting.
A Message from Ben Fury
I was writing a book on health, fitness and diet in 2009 when my house burned down in the Station Fire, along with 165,000 acres of my beloved Angeles National Forest. Since then, I've had a series of people needing help come through my life, that have upgraded and morphed my talents...
Seniors with chronic pain, falls, brittle bones, and stiff shrunken muscles.
Diabetics with out of control blood sugars, going blind, and having limbs lopped off.
Neurologically challenged people with spastic limbs and foggy brains.
Fat, listless, unhappy people with no idea how they got that way, seeing no way out of the darkness.
Each of them needing help in different ways, but all with an underlying theme of what works to help heal our conditions:
Seniors with chronic pain, falls, brittle bones, and stiff shrunken muscles.
Diabetics with out of control blood sugars, going blind, and having limbs lopped off.
Neurologically challenged people with spastic limbs and foggy brains.
Fat, listless, unhappy people with no idea how they got that way, seeing no way out of the darkness.
Each of them needing help in different ways, but all with an underlying theme of what works to help heal our conditions:
- Remove flour, sugar, beans, and heavily processed oils from our diet. Eat real food.
- Get strong.
- Get flexible.
- Stop ceding health responsibility to outside forces, and take charge of our own wellness.
- Only use truly evidence based medicine. Don't just pop the latest pill or get the latest surgery all the other people are doing. Be wary of the disease mongers in both the conventional and alternative camps.
- Find our "happy thoughts." Use the simple restoratives of sleep, play, and reflection, to let go of pain, find inner peace, and let in joy and purposeful outer direction.
The methods to accomplish these goals are varied, and I have both non-profit and for-profit ventures to share them.
Their websites are currently in development.
The for-profit is BenFury.com
The non-profit is PainRelieversUSA.org , whose mission statement is:
To move beyond pain management...
and learn to live pain free.
Feel free to write to me at: ben [at] benfury dot com
Their websites are currently in development.
The for-profit is BenFury.com
The non-profit is PainRelieversUSA.org , whose mission statement is:
To move beyond pain management...
and learn to live pain free.
Feel free to write to me at: ben [at] benfury dot com
Monday, August 20, 2012
The 2012 Atherosclerosis egg study: Plaque decreased as LDL increased with consumption of 2.3 eggs per week or more
A new study by David Spence and colleagues, published online in July 2012 in the journal Atherosclerosis (), has been gaining increasing media attention (e.g., ). The article is titled: “Egg yolk consumption and carotid plaque”. As the title implies, the study focuses on egg yolk consumption and its association with carotid artery plaque buildup.
The study argues that “regular consumption of egg yolk should be avoided by persons at risk of cardiovascular disease”. It hints at egg yolks being unhealthy in general, possibly even more so than cigarettes. Solid critiques have already been posted on blogs by Mark Sisson, Chris Masterjohn, and Zoe Harcombe (, , ), among others.
These critiques present valid arguments for why the key findings of the study cannot be accepted, especially the finding that eggs are more dangerous to one’s health than cigarettes. This post is a bit different. It uses the data reported in the study to show that it (the data) suggests that egg consumption is actually health-promoting.
I used the numbers in Table 2 of the article to conduct a test that is rarely if ever conducted in health studies – a moderating effect test. I left out the “egg-yolk years” variable used by the authors, and focused on weekly egg consumption (see Chris’s critique). My analysis, using WarpPLS (), had to be done only visually, because using values from Table 2 meant that I had access only to data on a few variables organized in quintiles. That is, my analysis here using aggregate data is an N=5 analysis; a small sample indeed. The full-text article is not available publicly; Zoe was kind enough to include the data from Table 2 in her critique post.
Below is the model that I used for the moderating effect test. It allowed me to look into the effect that the variable EggsWk (number of eggs consumed per week) had on the association between LDL (LDL cholesterol) and Plaque (carotid plaque). This type of effect, namely a moderating effect, is confusing to many people, because it is essentially the effect that a variable has on the effect of another variable on a third. Still, being confusing does not mean being less important. I should note that this type of effect is similar to a type of conditional association tested via Bayesian statistics – if one eats more eggs, what is the association between having a high LDL cholesterol and plaque buildup?

You can see what is happening visually on the graph below. The plot on the left side is for low weekly egg consumption. In it, the association between LDL cholesterol and plaque is positive – eating fewer eggs, plaque and LDL increase together. The plot on the right side is for high weekly egg consumption. In this second plot, the association between LDL cholesterol and plaque is negative – eating more eggs, plaque decreases as LDL increases. And what is the turning point? It is about 2.3 eggs per week.

So the “evil” particle, the LDL, is playing tricks with us; but thankfully the wonderful eggs come to the rescue, right? Well, it looks a bit like it, but maybe other foods would have a similar effect. In part because of the moderating effect discussed above, the multivariate association between LDL cholesterol and plaque was overall negative. This multivariate association was estimated controlling for the moderating effect of weekly egg consumption. You can see this on the plot below.

The highest amount of plaque is at the far left of the plot. It is associated with the lowest LDL cholesterol quintile. (So much for eggs causing plaque via LDL cholesterol eh!?) What is happening here? Maybe egg consumption above a certain level shifts the size of the LDL particles from small to large, making the potentially atherogenic ones harmless. (Saturated fat consumption, in the context of a nutritious diet in lean individuals, seems to have a similar effect.) Maybe eggs contain nutrients that promote overall health, leading LDL particles to "behave" and do what they are supposed to do. Maybe it is a combination of these and other effects.
The study argues that “regular consumption of egg yolk should be avoided by persons at risk of cardiovascular disease”. It hints at egg yolks being unhealthy in general, possibly even more so than cigarettes. Solid critiques have already been posted on blogs by Mark Sisson, Chris Masterjohn, and Zoe Harcombe (, , ), among others.
These critiques present valid arguments for why the key findings of the study cannot be accepted, especially the finding that eggs are more dangerous to one’s health than cigarettes. This post is a bit different. It uses the data reported in the study to show that it (the data) suggests that egg consumption is actually health-promoting.
I used the numbers in Table 2 of the article to conduct a test that is rarely if ever conducted in health studies – a moderating effect test. I left out the “egg-yolk years” variable used by the authors, and focused on weekly egg consumption (see Chris’s critique). My analysis, using WarpPLS (), had to be done only visually, because using values from Table 2 meant that I had access only to data on a few variables organized in quintiles. That is, my analysis here using aggregate data is an N=5 analysis; a small sample indeed. The full-text article is not available publicly; Zoe was kind enough to include the data from Table 2 in her critique post.
Below is the model that I used for the moderating effect test. It allowed me to look into the effect that the variable EggsWk (number of eggs consumed per week) had on the association between LDL (LDL cholesterol) and Plaque (carotid plaque). This type of effect, namely a moderating effect, is confusing to many people, because it is essentially the effect that a variable has on the effect of another variable on a third. Still, being confusing does not mean being less important. I should note that this type of effect is similar to a type of conditional association tested via Bayesian statistics – if one eats more eggs, what is the association between having a high LDL cholesterol and plaque buildup?

You can see what is happening visually on the graph below. The plot on the left side is for low weekly egg consumption. In it, the association between LDL cholesterol and plaque is positive – eating fewer eggs, plaque and LDL increase together. The plot on the right side is for high weekly egg consumption. In this second plot, the association between LDL cholesterol and plaque is negative – eating more eggs, plaque decreases as LDL increases. And what is the turning point? It is about 2.3 eggs per week.

So the “evil” particle, the LDL, is playing tricks with us; but thankfully the wonderful eggs come to the rescue, right? Well, it looks a bit like it, but maybe other foods would have a similar effect. In part because of the moderating effect discussed above, the multivariate association between LDL cholesterol and plaque was overall negative. This multivariate association was estimated controlling for the moderating effect of weekly egg consumption. You can see this on the plot below.

The highest amount of plaque is at the far left of the plot. It is associated with the lowest LDL cholesterol quintile. (So much for eggs causing plaque via LDL cholesterol eh!?) What is happening here? Maybe egg consumption above a certain level shifts the size of the LDL particles from small to large, making the potentially atherogenic ones harmless. (Saturated fat consumption, in the context of a nutritious diet in lean individuals, seems to have a similar effect.) Maybe eggs contain nutrients that promote overall health, leading LDL particles to "behave" and do what they are supposed to do. Maybe it is a combination of these and other effects.
Thursday, August 16, 2012
Ancestral Health Symposium 2012
I recently returned from AHS12 and a little side trip to visit family. The conference was hosted at Harvard University through the Harvard Food Law Society. Many thanks to all the organizers who made it happen. By and large, it went smoothly.
The science as expected ranged from outstanding to mediocre, but I was really encouraged by the presence and enthusiastic participation of a number of quality researchers and clinicians. The basic concept of ancestral health is something almost anyone can get behind: many of our modern health problems are due to a mismatch between the modern environment and what our bodies "expect". The basic idea is really just common sense, but of course the devil is in the details when you start trying to figure out what exactly our bodies expect, and how best to give it to them. I think our perspective as a community is moving in the right direction.
Read more »
The science as expected ranged from outstanding to mediocre, but I was really encouraged by the presence and enthusiastic participation of a number of quality researchers and clinicians. The basic concept of ancestral health is something almost anyone can get behind: many of our modern health problems are due to a mismatch between the modern environment and what our bodies "expect". The basic idea is really just common sense, but of course the devil is in the details when you start trying to figure out what exactly our bodies expect, and how best to give it to them. I think our perspective as a community is moving in the right direction.
Read more »
Tuesday, August 14, 2012
Ancestral Health Symposium 2012: Evolutionarily sound diets and lifestyles may revolutionize health care
The Ancestral Health Symposium 2012 was very interesting on many levels. Aaron Blaisdell and the team of volunteers really did a superb job at organizing the Symposium. Boston is a great city with an excellent public transportation system, something that is always great for meetings, and a great choice for the Symposium. Needless to say, so was Harvard. Even though the program was packed there were plenty of opportunities to meet and talk with several people during the breaks.
We had our panel “New Technologies and New Opportunities”, which Paul Jaminet moderated. The panelists were Chris Keller, Chris Kresser, Dan Pardi, and myself. The first photo below, by Bobby Gill, shows Chris Keller speaking; I am on the far left looking at the screen. The second photo, by Beth Mazur, shows all the panelists. The third photo, also by Bobby Gill, shows a group of us talking to Stephan Guyenet after his presentation.



I talked a bit toward the end of the panel about the importance of taking nonlinearity into consideration in analyses of health data, but ended up being remembered later for saying that “men are women with a few design flaws”. I said that to highlight the strong protective effect of being female in terms of health, which was clear from the model I was discussing.
There is a good evolutionary reason for the protective effect of being female. Evolution is a population phenomenon. Genes do not evolve; neither do individuals. Populations evolve through the spread or disappearance of genotypes. A healthy population with 99 men and 1 woman will probably disappear quickly, and so will its gene pool. A healthy population with 99 women and 1 man will probably thrive, even with the drag of inbreeding depression. Under harsh environmental conditions, the rate of female-to-male births goes up, in some cases quite a lot.
I was able to talk to, or at least meet briefly face-to-face with, many of the people that I have interacted with online on this blog and other blogs. Just to name a few: Miki Ben-Dor, Aaron Blaisdell, Emily Deans, Andreas Eenfeldt, Glenn Ellmers, Benjamin Gebhard, Stephan Guyenet, Dallas Hartwig, Melissa Hartwig, Paul Jaminet, Chris Keller, Chris Kresser, Mathieu Lalonde, Robert Lustig, Chris Masterjohn, Beth Mazur, Denise Minger, Jimmy Moore, Katherine Morrison, Richard Nikoley, Dan Pardi, Kamal Patel, David Pendergrass, Mark Sisson, Mary Beth Smrtic, J. Stanton, Carlos Andres Toro, and Grayson Wheatley.
It would have been nice to have Peter (from Hyperlipid) there, as I think a lot of the attendants are fans. I attended Jamie Scott’s very interesting talk, but ended up not being able to chat with him. This is a pity because we share some common experiences – e.g., I lived in New Zealand for a few years. I did have the opportunity to talk at some length with J. Stanton, who is an inspiration. It was also great to exchange some ideas with my panelists, Miki Ben-Dor, Emily Deans, Stephan Guyenet, Chris Masterjohn, Kamal Patel, and David Pendergrass. I wish I had more time to talk with Denise Minger, who is clearly a very nice person in addition to being very smart. Talking about a smart person, it was also nice chatting a bit with Richard Nikoley; a successful entrepreneur who is in the enviable position of doing what he feels like doing.
I could not help but notice a tendency among some participants (perhaps many, judging from online threads) to pay a lot of attention to how other people looked in a very judgmental way. That person is too fat, his/her face is too red, she/he looks too old etc. So was this supposed to be the Ancestral Health Pageant 2012? There is nothing wrong with looking good. But many people adopt an evolution-inspired lifestyle because they are quite unhealthy to start with. And this includes some of the presenters. It takes time to change one’s health, relapses occur, and no one is getting younger. Moreover, some of the presenters’ ideas and advice may have much more dramatic positive effects on people other than themselves, because of their own pre-existing conditions. The ideas and advice are still solid.
A message that I think this Symposium conveyed particularly well was that an evolutionarily sound diet and lifestyle can truly revolutionize our health care system. Robb Wolf’s talk in particular, based on his recent experience in Nevada with law enforcement officers, made this point very effectively. The title of the talk is “How Markets and Evolution Can Revolutionize Medicine”. One very interesting idea he put forth was that establishments like gyms could expand the range of support activities they offer their customers, officially becoming the beginning of the health care chain. There are already health insurance plans that offer premium reductions for those who go to gyms. Being part of the health care chain would be different and a significant step forward - diet and exercise are powerful "drugs".
One thing that caught me a bit off-guard was Robb’s strong advocacy of the use of a drug, namely metformin (a.k.a. glucophage); even preventively in some special cases, such as with sleep-deprived law enforcement officers. I have to listen to that talk again when it is up online, to make sure that I understood it correctly. It seems to me that changing the nature of shift work among law enforcement officers, at least partially, may be a better target; current practices appear not only to impair the officers’ health but also their effectiveness in law enforcement activities. Besides, I think we need to better understand the nature and functions of cortisol, which is viewed by many as a hormone that exists only to do us harm.
Sleep deprivation is associated with an elevation in cortisol production. Elevated cortisol levels lead over time to visceral fat accumulation, which promotes systemic inflammation. Systemic inflammation is possibly the root cause of most diseases of civilization. But cortisol itself has powerful anti-inflammatory properties, and visceral fat is generally easy to mobilize through intense exercise – probably one of the key reasons why we have visceral fat. I think we need to understand this situation a bit better before thinking about preventive uses of metformin, which nevertheless is a drug that seems to do wonders in the treatment of type 2 diabetes.
Beth Mazur was kind enough to put up a post with links to various Ancestral Health Symposium 2012 summary posts, as well as pictures. Paul Jaminet has a post with an insightful discussion of our panel at the Symposium.
We had our panel “New Technologies and New Opportunities”, which Paul Jaminet moderated. The panelists were Chris Keller, Chris Kresser, Dan Pardi, and myself. The first photo below, by Bobby Gill, shows Chris Keller speaking; I am on the far left looking at the screen. The second photo, by Beth Mazur, shows all the panelists. The third photo, also by Bobby Gill, shows a group of us talking to Stephan Guyenet after his presentation.



I talked a bit toward the end of the panel about the importance of taking nonlinearity into consideration in analyses of health data, but ended up being remembered later for saying that “men are women with a few design flaws”. I said that to highlight the strong protective effect of being female in terms of health, which was clear from the model I was discussing.
There is a good evolutionary reason for the protective effect of being female. Evolution is a population phenomenon. Genes do not evolve; neither do individuals. Populations evolve through the spread or disappearance of genotypes. A healthy population with 99 men and 1 woman will probably disappear quickly, and so will its gene pool. A healthy population with 99 women and 1 man will probably thrive, even with the drag of inbreeding depression. Under harsh environmental conditions, the rate of female-to-male births goes up, in some cases quite a lot.
I was able to talk to, or at least meet briefly face-to-face with, many of the people that I have interacted with online on this blog and other blogs. Just to name a few: Miki Ben-Dor, Aaron Blaisdell, Emily Deans, Andreas Eenfeldt, Glenn Ellmers, Benjamin Gebhard, Stephan Guyenet, Dallas Hartwig, Melissa Hartwig, Paul Jaminet, Chris Keller, Chris Kresser, Mathieu Lalonde, Robert Lustig, Chris Masterjohn, Beth Mazur, Denise Minger, Jimmy Moore, Katherine Morrison, Richard Nikoley, Dan Pardi, Kamal Patel, David Pendergrass, Mark Sisson, Mary Beth Smrtic, J. Stanton, Carlos Andres Toro, and Grayson Wheatley.
It would have been nice to have Peter (from Hyperlipid) there, as I think a lot of the attendants are fans. I attended Jamie Scott’s very interesting talk, but ended up not being able to chat with him. This is a pity because we share some common experiences – e.g., I lived in New Zealand for a few years. I did have the opportunity to talk at some length with J. Stanton, who is an inspiration. It was also great to exchange some ideas with my panelists, Miki Ben-Dor, Emily Deans, Stephan Guyenet, Chris Masterjohn, Kamal Patel, and David Pendergrass. I wish I had more time to talk with Denise Minger, who is clearly a very nice person in addition to being very smart. Talking about a smart person, it was also nice chatting a bit with Richard Nikoley; a successful entrepreneur who is in the enviable position of doing what he feels like doing.
I could not help but notice a tendency among some participants (perhaps many, judging from online threads) to pay a lot of attention to how other people looked in a very judgmental way. That person is too fat, his/her face is too red, she/he looks too old etc. So was this supposed to be the Ancestral Health Pageant 2012? There is nothing wrong with looking good. But many people adopt an evolution-inspired lifestyle because they are quite unhealthy to start with. And this includes some of the presenters. It takes time to change one’s health, relapses occur, and no one is getting younger. Moreover, some of the presenters’ ideas and advice may have much more dramatic positive effects on people other than themselves, because of their own pre-existing conditions. The ideas and advice are still solid.
A message that I think this Symposium conveyed particularly well was that an evolutionarily sound diet and lifestyle can truly revolutionize our health care system. Robb Wolf’s talk in particular, based on his recent experience in Nevada with law enforcement officers, made this point very effectively. The title of the talk is “How Markets and Evolution Can Revolutionize Medicine”. One very interesting idea he put forth was that establishments like gyms could expand the range of support activities they offer their customers, officially becoming the beginning of the health care chain. There are already health insurance plans that offer premium reductions for those who go to gyms. Being part of the health care chain would be different and a significant step forward - diet and exercise are powerful "drugs".
One thing that caught me a bit off-guard was Robb’s strong advocacy of the use of a drug, namely metformin (a.k.a. glucophage); even preventively in some special cases, such as with sleep-deprived law enforcement officers. I have to listen to that talk again when it is up online, to make sure that I understood it correctly. It seems to me that changing the nature of shift work among law enforcement officers, at least partially, may be a better target; current practices appear not only to impair the officers’ health but also their effectiveness in law enforcement activities. Besides, I think we need to better understand the nature and functions of cortisol, which is viewed by many as a hormone that exists only to do us harm.
Sleep deprivation is associated with an elevation in cortisol production. Elevated cortisol levels lead over time to visceral fat accumulation, which promotes systemic inflammation. Systemic inflammation is possibly the root cause of most diseases of civilization. But cortisol itself has powerful anti-inflammatory properties, and visceral fat is generally easy to mobilize through intense exercise – probably one of the key reasons why we have visceral fat. I think we need to understand this situation a bit better before thinking about preventive uses of metformin, which nevertheless is a drug that seems to do wonders in the treatment of type 2 diabetes.
Beth Mazur was kind enough to put up a post with links to various Ancestral Health Symposium 2012 summary posts, as well as pictures. Paul Jaminet has a post with an insightful discussion of our panel at the Symposium.
Saturday, August 4, 2012
Lorcaserin: the Latest FDA-approved Obesity Drug
The FDA recently approved a new drug called lorcaserin (brand name Belviq) for the treatment of obesity. Lorcaserin causes an average of 13 lbs (5.8 kg) of weight loss over a year, compared to 5 lbs (2.2 kg) for placebo (1), which is less than the other recently approved drug Qsymia (formerly Qnexa; topiramate/phentermine).
Learning about obesity drugs is always a good opportunity to gain insight into the mechanisms that underlie the development and reversal of obesity. If you've been following this blog for a while, you already have a pretty good guess what organ this new drug acts on. Make your guess and read on!
Read more »
Learning about obesity drugs is always a good opportunity to gain insight into the mechanisms that underlie the development and reversal of obesity. If you've been following this blog for a while, you already have a pretty good guess what organ this new drug acts on. Make your guess and read on!
Read more »
Thursday, August 2, 2012
Two Great Quotes About Obesity (technical)
By Dr. Hans-Rudolf Berthoud, from a recent paper, "The Neurobiology of Food Intake in an Obesogenic Environment" (1). I came across it because it cites my review paper (2). My perspective on obesity is similar to his. From the abstract:
Read more »
The modern lifestyle with its drastic changes in the way we eat and move puts pressure on the homoeostatic system responsible for the regulation of body weight, which has led to an increase in overweight and obesity. The power of food cues targeting susceptible emotions and cognitive brain functions, particularly of children and adolescents, is increasingly exploited by modern neuromarketing tools. Increased intake of energy-dense foods high in fat and sugar is not only adding more energy, but may also corrupt neural functions of brain systems involved in nutrient sensing as well as in hedonic, motivational and cognitive processing.And a nice one from the conclusions:
Read more »
Tuesday, July 31, 2012
The 14-percent advantage of eating little and then a lot: Putting it in practice
In my previous post I argued that the human body may react to “eating big” as it would to overfeeding, increasing energy expenditure by a certain amount. That increase seems to lead to a reduction in the caloric value of the meals during overfeeding; a reduction that seems to gravitate around 14 percent of the overfed amount.
And what is the overfed amount? Let us assume that your daily calorie intake to maintain your current body weight is 2,000 calories. However, one day you consume 1,000 calories, and the next 3,000 – adding up to 4,000 calories in 2 days. This amounts to 2,000 calories per day on average, the weight maintenance amount; but the extra 1,000 on the second day is perceived by your body as overfeeding. So 140 calories are “lost”.
The mechanisms by which this could happen are not entirely clear. Some studies contain clues; one example is the 2002 study conducted with mice by Anson and colleagues (), from which the graphs below were taken.

In the graphs above AL refers to ad libitum feeding, LDF to limited daily feeding (40 percent less than AL), IF to intermittent (alternate-day) fasting, and PF to pair-fed mice that were provided daily with a food allotment equal to the average daily intake of mice in the IF group. PF was added a control condition; in practice, the 2-day food consumption was about the same in AL, IF and PF.
After a 20-week period, intermittent fasting was associated with the lowest blood glucose and insulin concentrations (graphs a and b), and the highest concentrations of insulin growth factor 1 and ketones (graphs c and d). These seem to be fairly positive outcomes. In humans, they would normally be associated with metabolic improvements and body fat loss.
Let us go back to the 14 percent advantage of eating little and then a lot; a pattern of eating that can be implemented though intermittent fasting, as well as other approaches.
So, as we have seen in the previous post (), it seems that if you consume the same number of calories, but you do that while alternating between underfeeding and overfeeding, you actually “absorb” 14 percent fewer calories – with that percentage applied to the extra calorie intake above the amount needed for weight maintenance.
And here is a critical point, which I already hinted at in the previous post (): energy expenditure is not significantly reduced by underfeeding, as long as it is short-term underfeeding – e.g., about 24 h or less. So you don’t “gain back” the calories due to a possible reduction in energy expenditure in the (relatively short) underfeeding period.
What do 140 calories mean in terms of fat loss? Just divide that amount by 9 to get an estimate; about 15 g of fat lost. This is about 1 lb per month, and 12 lbs per year. Does one lose muscle due to this, in addition to body fat? A period of underfeeding of about 24 h or less should not be enough to lead to loss of muscle, as long as one doesn’t do glycogen-depleting exercise during that period ().
Sounds good? It actually gets better. Underfeeding tends to increase the body’s receptivity to both micronutrients and macronutrients. This applies to protein, carbohydrates, vitamins etc. For example, the activity of liver and muscle glycogen synthase is significantly increased by underfeeding (the scientific term is “phosphorylation”), particularly carbohydrate underfeeding, effectively raising the insulin sensitivity of those tissues.
The same happens, in general terms, with a host of other tissues and nutrients; often mediated by enzymes. This means that after a short period of underfeeding your body is primed to absorb micronutrients and macronutrients more effectively, even as it uses up some extra calories – leading to a 14 percent increase in energy expenditure.
There are many ways in which this can be achieved. Intermittent fasting is one of them; with 16-h to 24-h fasts, for example. Intermittent calorie restriction is another; e.g., with a 1/3 and 2/3 calorie consumption pattern across two-day periods. Yet another is intermittent carbohydrate restriction, with other macronutrients kept more or less constant.
If the same amount of food is consumed, there is evidence suggesting that such practices would lead to body weight preservation with improved body composition – same body weight, but reduced fat mass. This is what the study by Anson and colleagues, mentioned earlier, suggested ().
A 2005 study by Heilbronn and colleagues on alternate day fasting by humans suggested a small decrease in body weight (); although the loss was clearly mostly of fat mass. Interestingly, this study with nonobese humans suggested a massive decrease in fasting insulin, much like the mice study by Anson and colleagues.
Having said all of the above, there are several people who gain body fat by alternating between eating little and a lot. Why is that? The most likely reason is that when they eat a lot their caloric intake exceeds the increased energy expenditure.
And what is the overfed amount? Let us assume that your daily calorie intake to maintain your current body weight is 2,000 calories. However, one day you consume 1,000 calories, and the next 3,000 – adding up to 4,000 calories in 2 days. This amounts to 2,000 calories per day on average, the weight maintenance amount; but the extra 1,000 on the second day is perceived by your body as overfeeding. So 140 calories are “lost”.
The mechanisms by which this could happen are not entirely clear. Some studies contain clues; one example is the 2002 study conducted with mice by Anson and colleagues (), from which the graphs below were taken.
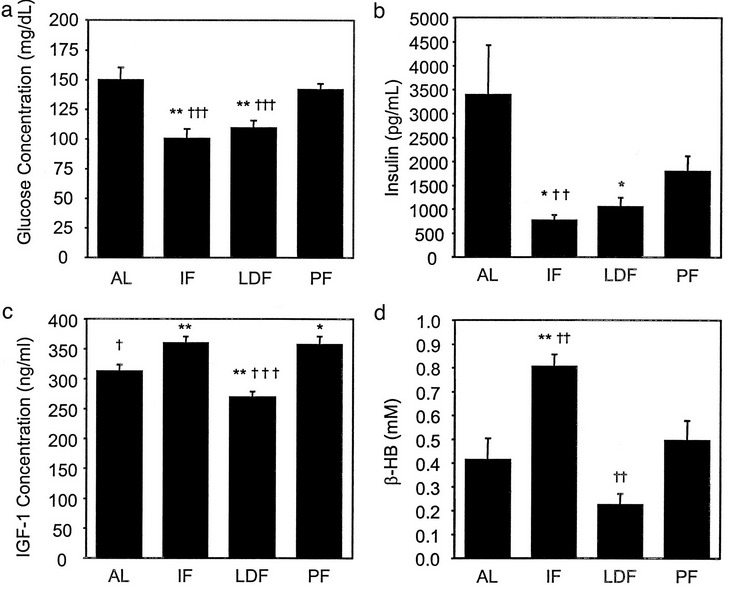
In the graphs above AL refers to ad libitum feeding, LDF to limited daily feeding (40 percent less than AL), IF to intermittent (alternate-day) fasting, and PF to pair-fed mice that were provided daily with a food allotment equal to the average daily intake of mice in the IF group. PF was added a control condition; in practice, the 2-day food consumption was about the same in AL, IF and PF.
After a 20-week period, intermittent fasting was associated with the lowest blood glucose and insulin concentrations (graphs a and b), and the highest concentrations of insulin growth factor 1 and ketones (graphs c and d). These seem to be fairly positive outcomes. In humans, they would normally be associated with metabolic improvements and body fat loss.
Let us go back to the 14 percent advantage of eating little and then a lot; a pattern of eating that can be implemented though intermittent fasting, as well as other approaches.
So, as we have seen in the previous post (), it seems that if you consume the same number of calories, but you do that while alternating between underfeeding and overfeeding, you actually “absorb” 14 percent fewer calories – with that percentage applied to the extra calorie intake above the amount needed for weight maintenance.
And here is a critical point, which I already hinted at in the previous post (): energy expenditure is not significantly reduced by underfeeding, as long as it is short-term underfeeding – e.g., about 24 h or less. So you don’t “gain back” the calories due to a possible reduction in energy expenditure in the (relatively short) underfeeding period.
What do 140 calories mean in terms of fat loss? Just divide that amount by 9 to get an estimate; about 15 g of fat lost. This is about 1 lb per month, and 12 lbs per year. Does one lose muscle due to this, in addition to body fat? A period of underfeeding of about 24 h or less should not be enough to lead to loss of muscle, as long as one doesn’t do glycogen-depleting exercise during that period ().
Sounds good? It actually gets better. Underfeeding tends to increase the body’s receptivity to both micronutrients and macronutrients. This applies to protein, carbohydrates, vitamins etc. For example, the activity of liver and muscle glycogen synthase is significantly increased by underfeeding (the scientific term is “phosphorylation”), particularly carbohydrate underfeeding, effectively raising the insulin sensitivity of those tissues.
The same happens, in general terms, with a host of other tissues and nutrients; often mediated by enzymes. This means that after a short period of underfeeding your body is primed to absorb micronutrients and macronutrients more effectively, even as it uses up some extra calories – leading to a 14 percent increase in energy expenditure.
There are many ways in which this can be achieved. Intermittent fasting is one of them; with 16-h to 24-h fasts, for example. Intermittent calorie restriction is another; e.g., with a 1/3 and 2/3 calorie consumption pattern across two-day periods. Yet another is intermittent carbohydrate restriction, with other macronutrients kept more or less constant.
If the same amount of food is consumed, there is evidence suggesting that such practices would lead to body weight preservation with improved body composition – same body weight, but reduced fat mass. This is what the study by Anson and colleagues, mentioned earlier, suggested ().
A 2005 study by Heilbronn and colleagues on alternate day fasting by humans suggested a small decrease in body weight (); although the loss was clearly mostly of fat mass. Interestingly, this study with nonobese humans suggested a massive decrease in fasting insulin, much like the mice study by Anson and colleagues.
Having said all of the above, there are several people who gain body fat by alternating between eating little and a lot. Why is that? The most likely reason is that when they eat a lot their caloric intake exceeds the increased energy expenditure.
Subscribe to:
Comments (Atom)