Canudos was located in the Brazilian sertão, an inhospitable semi-arid region in the northeastern part of the country. The inhabitants of Canudos were the sertanejos. The term jagunço was used to refer to the males, especially the outlaws. Many of the sertanejos lived in semi-starvation, in poor sanitary conditions, and with very limited (if any) access to healthcare. Infant mortality was very high at the time. Those who reached adulthood were typically of small stature, and very thin; not lean, thin – often described as “skin and bones”.
Below is what a typical young jagunço would look like at the time of the War of Canudos. (Some authors differentiate between jagunços and cangaceiros based on small differences in cultural and dress traditions; e.g., the hat in the photo is typical of cangaceiros.) The jagunços tended to be the best fed among the sertanejos. They were also known as cold-blooded killers. The photo is a cropped version of the original one; the grizzly original is at the top of a recent blog post by Juan Pablo Dabove (). The blog post discusses Vargas Llosa’s historical fiction book based on the War of Canudos, the masterpiece titled “The War of the End of the World” ().

Jorge Mario Pedro Vargas Llosa, a Peruvian-Spanish writer and politician, was the recipient of the 2010 Nobel Prize in Literature; “The War of the End of the World” is considered one of his greatest literary achievements. Euclides da Cunha wrote the most famous non-fictional account on the War of Canudos, another masterpiece that has been called “Brazil’s greatest book”, titled “Rebellion in the Backlands” (). The Portughese title is “Os Sertões”. Vargas Llosa’s book is based on da Cunha’s.
Sergio Rezende’s movie, “Guerra de Canudos” (), is a superb dramatization of the War of Canudos. I watched this movie after reading Vargas Llosa’s and da Cunha’s books, and was struck by two things: (a) the outstanding performances, especially by José Wilker, Cláudia Abreu, Marieta Severo, and Paulo Betti; and (b) the striking resemblance of the latter (Betti) to Royce Gracie (), a very nice man whom I interviewed () for my book on compensatory adaptation (), and who is no stranger to Ultimate Fighting Championship and mixed martial arts fans ().
In a nutshell, the War of Canudos went more or less like this. There were four military campaigns against the settlement. The third was a major one, led by one of Brazil’s most accomplished military leaders at the time, Colonel Antônio Moreira César. The jagunços, resorting to guerrilla warfare, fought off the government troops in the first three. The fourth, led by General Arthur Oscar de Andrade Guimarães, saw the jagunços defeated in a war of attrition primarily due to lack of access to food and water, after heavy losses among government troops. At the end, nearly all of the surviving jagunços were executed, by knife – to their absolute horror, and the perverse pleasure of the executioners bent on revenge, as the victims believed that they would not go to heaven if their lives were ended by knife, even against their will.
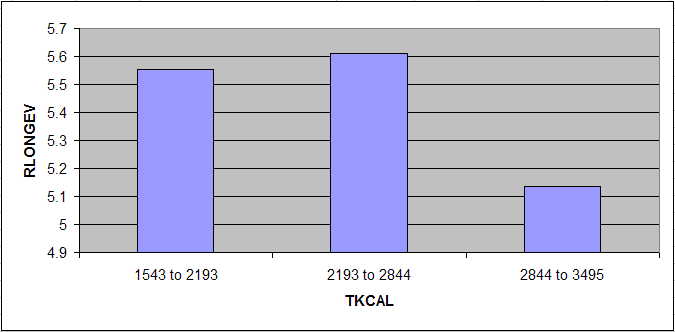
Ned, what is your point regarding health!?
After going through numerous sources, paper-based and online, academic and non-academic, I am convinced that a significant number of the survivors of the Canudos War lived to their 90s and beyond. This conclusion is based chiefly on comparisons of various dates, especially of interviews with survivors. No single source dedicated to this particular health-related aspect of the War of Canudos seems to exist. There is a video clip that shows some of the survivors (), speaking in Portuguese, with their ages shown in subtitles (“years”, in Portuguese, is “anos”). One of them, a man, is listed as being a supercentenarian.
In modern USA those who live to the age of 90 and beyond are outliers. Less than 2 percent of the population reach the age of 90 (). Most of them are women. My impression is that among the survivors of the War of Canudos, the 90+ percentage was at least 5 times higher; even with access to sanitation and healthcare in modern USA being much better at any age.
If my impression is correct, how can it be explained?
I think that some of the readers of this blog will be tempted to explain the high longevity based on calorie restriction. But the empirical evidence suggests that poor nutrition, in terms of micronutrients and macronutrients, is associated with increased mortality, not the other way around (, , ). Mortality due to poor nutrition is frequently from infectious diseases, in the young and the old. Degenerative diseases are widespread among the overnourished, not the well nourished, and kill mostly at later ages. It is not uncommon for infectious diseases to “mask” as degenerative diseases – e.g., viral diabetes ().
Often people point at hunter-gatherer populations and argue that they are healthy because of their low calorie intake. But mortality from infectious diseases among hunter-gatherers is very high, particularly in children. Others point to the absence of industrial foods engineered for overconsumption, which I think is definitely a factor in terms of degenerative diseases. Some say that a main factor is retention of lean body mass as one ages, referring mostly to muscle tissue, a hypothesis to which the case of the sertanejos poses a problem – what lean body mass!? And, on top of all of their problems, the sertanejos regularly faced long droughts, which may be why they typically had a “dry” look.
Yet others point to low stress. It is reasonable to think that stress is a mediating factor in the development of many modern diseases. Still, the sertanejos living in Canudos have had to endure quite a lot of stress, before and after the War of Canudos. In fact, the depictions of their lives at around the time of the War of Canudos suggest very stressful, miserable lives, prior to the conflict; which in part explains the early success of a religious settlement where life was marginally better.
By the way, the traditional Okinawans have also endured plenty of stress (), and they have had the highest longevity rates in recorded history. Food scarcity has frequently been combined with stress in their case, as with many other long-living groups. Causality is complex here, probably changing direction in different subsets of the data, but I have long suspected that the combination of stress and overnourishment is a particular unnatural one, to which humans are badly maladapted.
A main factor is almost always forgotten: the effective immune systems of those who have been subjected to starvation, poor sanitation, lack of healthcare, and other challenges – especially in childhood – and survived to adulthood. And here some counterintuitive things can happen. For example, someone may be very sickly early in life and barely survive childhood, and then become very resistant to infectious diseases later, thus appearing to be very healthy, to the surprise of relatives and friends who remember “that sickly child”. Immunocompetence is something that the body builds up in response to exposure.
As they say in northeastern Brazil, in characteristic drawl: “Ol’ sihtaneju ain’t die easy”.